Translate this page into:
A cadaveric feasibility study for a staged musculocutaneous to medial cord nerve transfer for restoration of hand function following infraclavicular brachial plexus injury
2 Department of Clinical Neurophysiology, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK
3 Department of Anaesthetics, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK
4 Birmingham Hand Centre, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK
Corresponding Author:
Daniel N Guerero
Peripheral Nerve Injury Service, Birmingham Hand Centre, University Hospitals NHS Foundation Trust, 6th Floor Nuffield House, Mindelsohn Way, Edgbaston, B15 2WB
UK
danielguerero@hotmail.com
| How to cite this article: Guerero DN, Guy IA, Shirley C, Edwards C, Power DM. A cadaveric feasibility study for a staged musculocutaneous to medial cord nerve transfer for restoration of hand function following infraclavicular brachial plexus injury. J Musculoskelet Surg Res 2019;3:104-109 |
Abstract
Objectives: Axonotmetic medial cord injury results in poor functional hand outcomes due to paralysis of long finger flexors and intrinsic hand muscles. The current management techniques have been reported to yield minimal functional recovery. This study aimed to determine the feasibility of a staged musculocutaneous nerve (MCN) to medial cord nerve transfer using the medial antebrachial cutaneous nerve (MACN) as an in situ reversed vascularized graft for the restoration of hand function in infraclavicular brachial plexus injury. The medial cord targets to be investigated include the nerve to flexor digitorum profundus (FDP), the deep branch of the ulnar nerve (DBUN), and the anterior interosseous nerve (AIN). Methods: Limb measurements were conducted on four fresh cadaveric upper limbs. Each upper limb was dissected by a peripheral nerve surgeon to expose the MACN, the nerve to FDP, the DBUN, and the AIN. The length of the MACN and the distance from the origin of each nerve to recognized forearm bone landmarks were measured. The surgical demonstration of the two-stage nerve transfer was demonstrated on a formalin-fixed upper extremity. Results: The mean graft length of the MACN was 223 mm (range: 179–295 mm). This was sufficient to bridge the calculated mean nerve gap to the nerve to FDP (88 mm, range: 79–101 mm) and DBUN (214 mm, range: 176–247 mm). The mean nerve gap to the AIN (228 mm, range: 201–252 mm) was greater than the mean MACN graft length. Conclusions: Motor nerve transfer of the brachialis muscle branch of the MCN to the medial cord using an interposed MACN graft was shown to allow tension-free neurorrhaphy formation with the nerve to FDP.
Introduction
The medial cord of the brachial plexus provides motor innervation to the muscles of both the distal ulnar nerve (ULN) and median nerve distributions. Its innervation territory includes the long finger flexors of the anterior forearm as well as the intrinsic muscles of the hand. High-grade injury of the medial cord is associated with inferior outcomes compared to the lateral and posterior cords due to long reinnervation distances, resulting in poor neural reinnervation.[1],[2]
Infraclavicular injuries of the medial cord with ulnar territory functional deficit have been reported to yield the lowest rates of useful functional recovery.[3] A long-term follow-up study by Gutkowska et al. reported that the approach of initial neurolysis with delayed distal nerve transfer if necessary for infraclavicular brachial plexus injury (BPI) yielded good rates of useful recovery in the majority of nerve distributions, with the exception of the ulnar territory.[4] Kosiyatrakul et al. concluded that the motor recovery for infraclavicular BPI is complete or nearly complete in all cases, with the exception of medial cord intrinsic function of the hand.[5] Hems and Mahmood[1] also reported that only two out of their 18 patients had full ulnar recovery.
Hand and finger function is of pivotal importance and as such innovation is required in the management of these cases. This study aimed to test the anatomical feasibility of a novel reconstructive procedure for the restoration of medial cord function in this patient group. This conceptual technique involves the use of the medial antebrachial cutaneous nerve (MACN) in the upper arm as an in situ reversed vascularized graft using the musculocutaneous nerve to brachialis (MCN BR) as the donor in a two-staged nerve transfer procedure [Figure - 1].
![[Figure - 1]](#fig_SaudiOrthopJ_2019_3_1_104_252390_f1.jpg){kind=link}
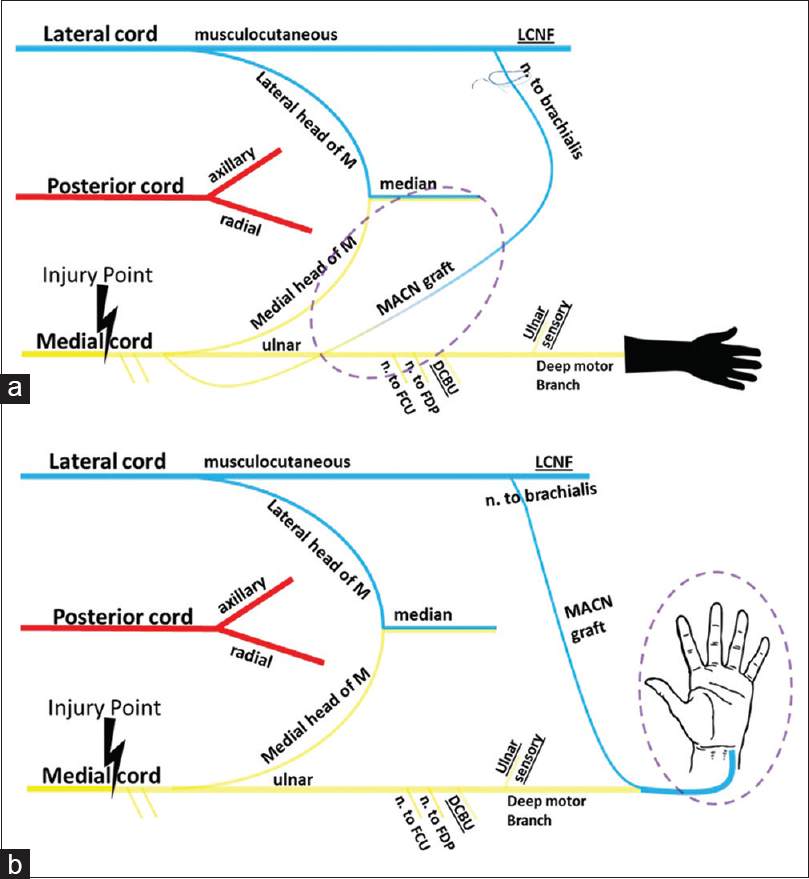 |
| Figure 1: Schematic Illustration of the novel conceptual procedure for the restoration of hand function in medial cord brachial plexus injury patients. (a) Stage 1 - The musculocutaneous nerve to brachialis-distal medial antebrachial cutaneous nerve loop is formed. The musculocutaneous nerve to brachialis is used as a donor to reinnervate the in situ reversed vascularized medial antebrachial cutaneous nerve graft. (b) Stage 2 - The medial antebrachial cutaneous nerve limb of the donor graft loop is sectioned proximally and transferred to reinnervate distal medial cord targets for the restoration of hand function |
Materials and Methods
Four fresh cadaveric arms were dissected by one of three trained peripheral nerve surgeons. All measurements were taken by two independent researchers. Arm and forearm lengths were measured using a ruler, whereas nerve lengths were measured using a digital vernier caliper micrometer accurate to 0.1 mm. All dissections and measurements were followed a predesigned protocol and all cadaveric materials were handled in accordance with the Human Tissue Act and local policies. Recorded values were analyzed using Microsoft Excel. All specimens included in the study had no evidence of gross pathology, previous surgical intervention, or previous trauma. The demographic data of the included cadavers were not made available to the research team for analysis.
Dissection technique
The cadaveric arms were placed supine in the anatomical position for the dissection. The medial bicipital sulcus was palpated, and a longitudinal incision was made along this axis. The superficial skin incision started at 3 cm proximal to the medial epicondyle and extended for a further 10 cm proximally. The underlying subcutaneous tissue was carefully dissected to identify the basilic vein. Several anatomical studies advocate identifying the basilic vein before the MACN as both pierce the deep fascia of the arm at the basilic hiatus to enter the subcutaneous tissue of the distal or midbrachium.[6],[7] Knowledge of this relatively consistent anatomical association was used to identify the MACN.[6],[8] Once identified, the MACN was traced proximally into the deep compartment of the arm to its point of origination from the medial cord in the axilla.
A second skin incision was created on the ventral forearm along the line connecting the medial epicondyle to the pisiform bone. This was subsequently extended to connect to the distal end of the previous incision. The MACN was dissected and traced distally within this incision beyond its branching point into anterior and posterior branches. Its main anterior branch was identified and dissected using knowledge of its typical path. It is reported to cross the elbow between the medial epicondyle and biceps tendon and usually travels anterior to the cubital vein to extend distally in the subcutaneous tissue overlying the flexor carpi ulnaris muscle and tendon.[6],[9] This was traced distally until it bifurcated into branches that were deemed too small for coaptation. The length of the MACN was measured from its point of origination in the axilla to the most distal point suitable for coaptation [Figure - 2].
![[Figure - 2]](#fig_SaudiOrthopJ_2019_3_1_104_252390_f2.jpg){kind=link}
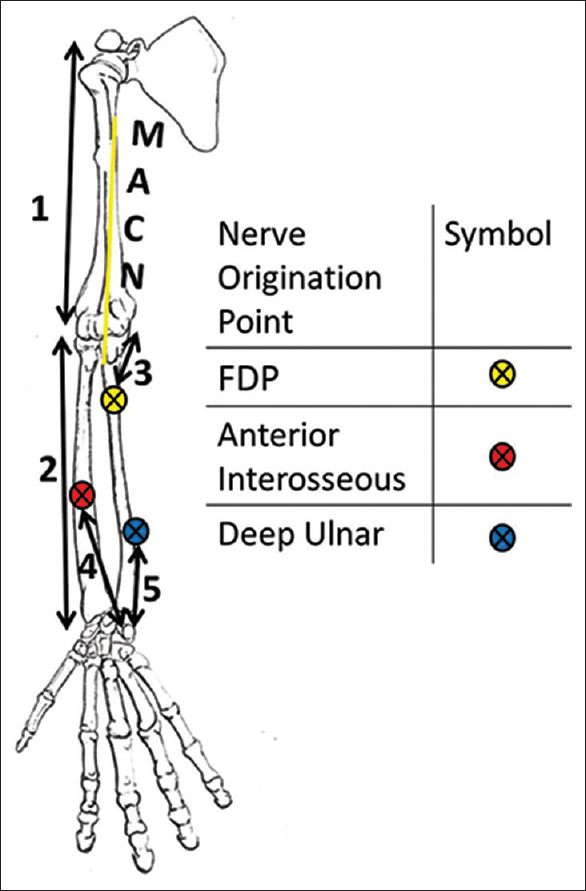 |
| Figure 2: Illustration showing the various measurements taken |
A third incision was made to open the arcuate ligament of Osborne overlying the cubital tunnel. The distal end of this incision was connected to the incision on the proximal forearm. The ULN was identified in the cubital tunnel and dissected from this point to just proximal to the wrist crease where it bifurcated into the superficial and deep branches of the ULN. Its branch to the flexor digitorum profundus (FDP) was identified, and its distance from the medial epicondyle was measured [[Figure - 2]: Number 3]. The median nerve was identified in the antecubital fossa and dissected distally exposing the anterior interosseous nerve (AIN) origin from its radial side. The length from the anterior interosseous trunk to the pisiform bone was measured [[Figure - 2]: Number 4].
A Taleisnik incision was made 6–7 mm medially to the thenar crease and was extended proximally in a zigzag manner such that it curved medially at the distal wrist crease and radially at the proximal wrist crease.[10] The proximal end of this zigzag incision was connected to the previous incision made on the volar surface of the forearm to the pisiform bone. Superficial dissection was performed at the distal part of the incision, and the palmar fascia and palmar carpal ligament were identified and dissected. The neurovascular bundle was marked with a silastic loop and mobilized medially to expose the ULN within the hand. The hook of the hamate and the muscle fascia of the hypothenar eminence were used to identify the point at which the deep motor branch of the ULN separated from the main ULN. ULN dissection was continued proximally until the point of take-off of the dorsal cutaneous branch was clearly identified. The cleavage plane between the sensory groups and the interdigitating motor fascicular group was identified, and internal neurolysis of the main ulnar trunk was carried out in a retrograde direction to separate the motor fascicle from the sensory fascicles. These are distinct functional units from Guyon's canal proximally to the take-off of the dorsal branch of the ULN 7 cm proximal to the pisiform. Beyond this point, the neurolysis may be limited by the presence of interfascicular branching.[11] The distance from the pisiform bone to the most distal interfascicular branch of the ULN was measured [[Figure - 2]: Number 5].
To assess the correlation between limb length and reinnervation distance, the linear distance of all included cadaveric limbs was measured. The distance from the lateral acromion to the lateral epicondyle was measured with the arm in a neutral position and was taken as the arm length [[Figure - 2]: Number 1]. Limb elbows were flexed to 90° and the distance from the lateral epicondyle to the radial styloid process tip of each limb was measured as the forearm length [[Figure - 2]: Number 2]. Total limb length was taken as the sum of these measurements.
Cadaveric surgical demonstration
A similar surgical demonstration procedure was carried out on a formalin-fixed upper extremity. The cadaveric arm was placed supine in the anatomical position for the dissection. An incision was made along the medial bicipital sulcus along the mid-portion of the medial arm. The skin and subcutaneous tissue were retracted, and a similar incision was made into the underlying brachial fascia. The biceps muscle was retracted and both the MCN and ULN were identified and dissected from surrounding connective tissue within the anterior compartment. The MCN BR was identified and dissected distally into the muscle before sectioning. The anterior branch of MACN was identified by making a longitudinal incision 2 cm anterior and 3 cm distal to the medial epicondyle. The MACN was dissected distally until it branched into cutaneous branches that were too small for coaptation. It was sectioned at this point and the proximal stump of this distal end was coapted to the previously sectioned MCN BR to form an end-to-end neurorrhaphy. Each of the previously identified medial cord targets was dissected and tagged with silastic loops as previously described. The MCN BR-MACN graft loop was traced proximally along its MACN limb and sectioned at the point of origination of the MACN from the medial cord to form a free nerve graft. The free proximal end of the MACN was approximated and coapted to determine the feasibility of tension-free neurorrhaphy with each of the previously identified distal motor nerve targets.
Results
The mean forearm and arm lengths were 248 mm and 301 mm, respectively, giving a mean upper limb length of 549 mm. The measured lengths facilitated the calculation of the required reinnervation distance for each of the desired medial cord targets [Table - 1]. Reinnervation ratios for each motor target were also calculated by dividing the required nerve gap by the total limb length [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2019_3_1_104_252390_t4.jpg){kind=link}

The mean length of the MACN (223 mm) was consistent with several studies, which reported that approximately 20 cm of MACN can be harvested as a free nerve graft.[8],[9],[12] The average length of MACN graft was greater than the average nerve gap to be bridged to reinnervate the FDP and deep branch of the ULN (DBUN). The individual measurements indicated that the MACN graft was long enough in each arm to comfortably form tension-free neurorrhaphies with the FDP motor branch. The individual measurements indicated that tension-free neurorrhaphy to the AIN and DBUN would only be feasible in one of the four specimens. Surgical demonstration was consistent with the cadaveric feasibility study, and the graft was easily coapted to form a tension-free neurorrhaphy with the nerve to ulnar FDP but insufficient to reach the DBUN or AIN [Figure - 3].
![[Figure - 3]](#fig_SaudiOrthopJ_2019_3_1_104_252390_f3.jpg){kind=link}
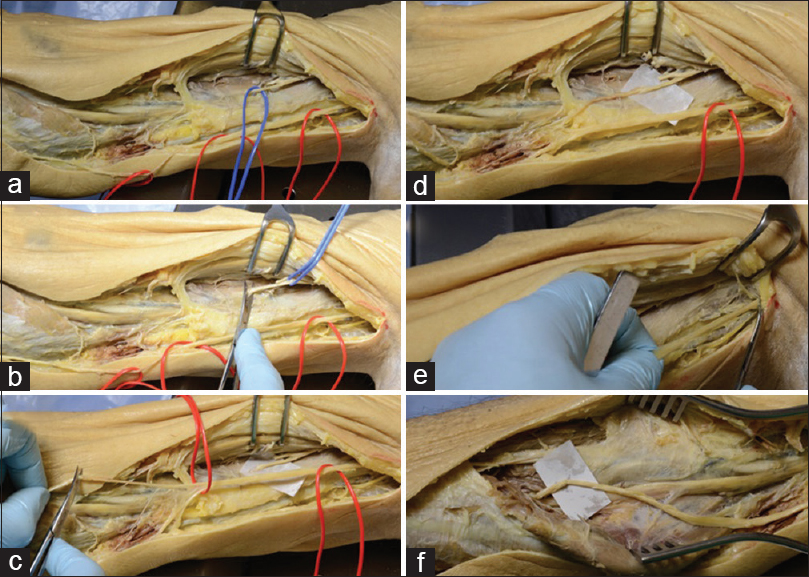 |
| Figure 3: Cadaveric images of the demonstrated theoretical procedure. (a) The medial antebrachial cutaneous nerve (red) and musculocutaneous nerve to brachialis (blue) were identified and dissected. (b) The musculocutaneous nerve to brachialis (blue) was sectioned distally. (c) The medial antebrachial cutaneous nerve (red) was sectioned distally. (d) The medial antebrachial cutaneous nerve (red) and musculocutaneous nerve to brachialis were coapted to form a neurorrhaphy. (e) The medial antebrachial cutaneous nerve limb of the donor graft loop was sectioned proximally. (f) The musculocutaneous nerve to brachialis-medial antebrachial cutaneous nerve nerve graft was rotated distally and coapted to the nerve to ulnar flexor digitorum profundus |
Discussion
Medial cord injury is recognized to have poor functional outcomes, and reconstructive options are limited with no standard surgical nerve transfer techniques available for restoration of distal medial cord function. In cases of medial cord injury with lateral or posterior cord sparing, the distance between potential donor motor branches and possible denervated medial cord targets is so great that reconstruction with nerve transfers, even if performed acutely after injury, may not provide sufficient time for successful reinnervation.
Denervated muscles undergo a pathological process whereby they lose their ability to be reinnervated. This process begins at the point of denervation and is typically completed within 12 months of denervation. Axons must rescue the denervated musculature before completion of this process for there to be any chance of functional recovery. This is problematic in the medial cord injury because it supplies the most distal musculature of the upper limb while being located near the axilla. Furthermore, nerve axons only exhibit a maximal regenerative rate of 1–2 mm/day and the small intrinsic muscles of the hand have been reported to have an increased affinity for degeneration, thereby shortening the available rescue window. These muscles require rapid reinnervation to stand a chance of making a good functional recovery.[13]
The conceptual procedure involved the use of the MACN as an in situ reversed vascularized graft using the MCN BR as the donor in a staged nerve transfer procedure to reinnervate distal medial cord motor targets. It was designed with the aim of salvaging hand muscle function before the collapse of their intramuscular neural network and as such every aspect of its design was selected to minimize the required reinnervation time. Axonal regeneration through a graft of maximum 22 cm in length is expected to take approximately 6 months and a further 3 months would be required for regeneration to the motor end plates.
First, the procedure employs basic nerve transfer principles to minimize the required axonal regeneration distance. The donor nerve selected was the MCN BR. This nerve is a branch of the lateral cord and would therefore retain function in isolated medial cord injury. Even though the brachialis is considered to be the primary flexor of the elbow, it has been shown to result in little to no donor morbidity when utilized as a nerve donor.[14] This is because it serves a redundant function to biceps. The MCN BR is a powerful motor axon donor in the upper limb and can potentially be an adequate supply of axons for medial cord targets despite the anticipated losses across the required neurorrhaphy.[15],[16] The MCN BR has also been documented to have a synergistic effect when used for reinnervation of long finger flexors, indicating that patients would have earlier cortical motor remapping in the postoperative phase of rehabilitation.[17]
The conceptual technique also uses the MACN as an autograft to bridge the nerve gap between the donor nerve and recipient medial cord targets. The MACN was selected for several reasons. First, the MACN has frequently been used in nerve grafting and has been reported to yield successful results, which were comparable to other grafts in several studies.[6],[8] Second, the main anterior branch of the MACN has a consistent subcutaneous course and distribution, making it easy to identify and isolate with minimal dissection.[6],[18] It is also located within the same operative field as the MCN BR, avoiding the need for additional incisions[19] and facilitating the use of regional anesthesia.[18] The use of the MACN has been reported to be associated with varying degrees of donor site morbidity. Several authors have reported minimal functional donor morbidity;[8],[18],[19] however, Higgins et al. contradicted this view by highlighting that the resulting sensory deficit in MACN grafting is more notable than in some alternatives, citing significant sensory losses to the elbow and posterior proximal forearm.[20] Some reports also indicated that this can be quite bothersome if neuroma formation occurs.[6],[9],[21],[22]
The proximity of the MACN to the MCN BR also facilitated in situ grafting in the reversed orientation. Reversing graft orientation has been reported to yield a higher proportion of axons regenerating to the distal stump and greater conduction velocities across branched grafts.[23] The majority of grafts used clinically will be long enough to contain branches and the MACN is no exception. It is documented in the literature to have a major branching point after it pierces the basilic hiatus and as such the decision was made to utilize this technique in this novel procedure.[12]
A two-stage procedure was favored for a number of reasons. The first stage of the procedure requires very little dissection of the MACN as the MCN BR branch is only coapted to the distal end of its main anterior branch. This portion of the nerve could be identified in isolation by making a longitudinal incision 2 cm anterior and 3 cm distal to the medial epicondyle as described by Nunley et al.[18] The entirety of the nerve would only be dissected from its underlying tissue bed in the second stage procedure. This implies that the graft would have optimal vascularity for the duration of the period of axonal regeneration through it. Nutrient provision is a strong determinant of outcome in nerve grafting.[24] For the majority of axonal regeneration, the MACN autograft is left in situ and experiences similar conditions to that of a vascularized nerve graft. Several studies have demonstrated superior results with vascularized nerve grafts.[25],[26],[27],[28]
Choosing a staged procedure also facilitated retaining the standard practice of observing nerve injury for spontaneous recovery for 3 months. Previously described single stage nerve transfer procedures would require sectioning the medial cord pathway quite early, thereby relinquishing the chance of spontaneous recovery.[29],[30] The first stage of this procedure can be performed early after injury in suspected high-grade medial cord injury before the outcome is fully determined to allow progressive retrograde reinnervation in readiness for later distal rotation to a denervated target. The ingenuity of this staged design lies in the adaptability of the procedure to the variable spontaneous recovery of the medial cord pathway without any loss of axonal regeneration time. The procedure is designed such that reinnervation through the MACN graft occurs while the original medial cord pathway is still intact. Should proximal branches of the medial cord recover, for example, the branch to Flexor Carpi Ulnaris (FCU) or FDP, then the graft created in stage one can be coapted to target reinnervation further down the medial cord pathway. In the unlikely scenario that the total medial cord recovers, the banked graft could be abandoned or used to reinnervate the brachialis, with the patient experiencing very limited morbidity after only undergoing the stage one procedure. Furthermore, the sectioning and coaptation of the MACN would yield no donor site morbidity in patients with total medial cord injury.
One major limitation of this study's design is the limited sample of cadaveric arms that were dissected. The effect of age, ethnicity, or sex on the measured lengths could not be investigated. Given the small sample size, the reported reinnervation ratios would require further validation. These ratios of required reinnervation distance to total limb length can be used to estimate the required graft length for a specific motor target in an individual patient. This would be achieved by simply measuring their upper limb length and multiplying by the specific reinnervation ratio. Knowledge of the required graft length and the conventional rate of axonal regeneration can be used to plan the timing of the second stage procedure.
It should be noted that another nerve transfer procedure was hypothesized applying similar nerve transfer principles discussed in this study. This procedure involved the use of the nerves to supinator as the donor motor nerves with a lateral cutaneous nerve of the forearm graft. It can be performed alongside this procedure in the small subset of patients who suffer isolated medial cord injury. The concurrent use of both procedures would facilitate the specific targeting of multiple denervated medial cord territories with more motor axons, potentially leading to greater functional recovery.
Conclusions
A conceptual nerve transfer technique was proven to be feasible by means of a cadaveric feasibility study and was subsequently demonstrated in a cadaveric surgical demonstration where tension-free neurorrhaphies were successfully performed at the nerve to FDP. The MCN BR-MACN graft loop was not long enough for coaptation at the DBUN or AIN after separation of these nerve structures from their main trunks. However, these nerve territories can still be targeted via coaptation of the graft to their fascicle structures within their derivative trunks as distally as the graft permits.
Ethical considerations
Cadaveric arms were provided by the Anatomy Departments at Keele University School of Medicine and the University of Birmingham. The consent for the use of the cadavers in scientific research was obtained from these departments. All dissection was conducted in accordance with local protocols and the Human Tissue Act. Appropriate consent was also obtained for the capture and publication of photographs.
Acknowledgement
We thank Professor Joanne Wilton for the support provided and inspiration that she gave to us all, may she rest in peace.
Financial support and sponsorship
This study was supported by the Department of Anatomy at the University of Birmingham.
Conflicts of interest
There are no conflicts of interest.
Author's contributions
DNG was involved in data collection, analysis, and interpretation and also wrote the final draft of the article. IAG was also involved in all aspects of data management; that is, data collection, organisation, analysis, and interpretation. CS and CE supported DMP in the design of the study, aided in data analysis, and provided logistic support. DMP conceived the novel procedure, designed the study, and collected data. All authors have critically reviewed and approved the final draft and accept responsibility for the content and similarity index of the manuscript.
| 1. | Hems TE, Mahmood F. Injuries of the terminal branches of the infraclavicular brachial plexus: Patterns of injury, management and outcome. J Bone Joint Surg Br 2012;94:799-804. [Google Scholar] |
| 2. | Birch R. Surgical Disorders of the Peripheral Nerves. London: Springer; 2011. [Google Scholar] |
| 3. | Siqueira MG, Martins RS. Surgical treatment of adult traumatic brachial plexus injuries: An overview. Arq Neuropsiquiatr 2011;69:528-35. [Google Scholar] |
| 4. | Gutkowska O, Martynkiewicz J, Mizia S, Bąk M, Gosk J. Results of operative treatment of brachial plexus injury resulting from shoulder dislocation: A study with A long-term follow-up. World Neurosurg 2017;105:623-31. [Google Scholar] |
| 5. | Kosiyatrakul A, Jitprapaikulsarn S, Durand S, Oberlin C. Recovery of brachial plexus injury after shoulder dislocation. Injury 2009;40:1327-9. [Google Scholar] |
| 6. | Masear VR, Meyer RD, Pichora DR. Surgical anatomy of the medial antebrachial cutaneous nerve. J Hand Surg Am 1989;14:267-71. [Google Scholar] |
| 7. | Benedikt S, Parvizi D, Feigl G, Koch H. Anatomy of the medial antebrachial cutaneous nerve and its significance in ulnar nerve surgery: An anatomical study. J Plast Reconstr Aesthet Surg 2017;70:1582-8. [Google Scholar] |
| 8. | Haller JR, Shelton C. Medial antebrachial cutaneous nerve: A new donor graft for repair of facial nerve defects at the skull base. Laryngoscope 1997;107:1048-52. [Google Scholar] |
| 9. | Slutsky JD. A practical approach to nerve grafting in the upper extremity. Atlas Hand Clin 2005;10:73-92. [Google Scholar] |
| 10. | Brown JM, Yee A, Mackinnon SE. Distal median to ulnar nerve transfers to restore ulnar motor and sensory function within the hand: Technical nuances. Neurosurgery 2009;65:966-77. [Google Scholar] |
| 11. | Atkins SE, Logan B, McGrouther DA. The deep (motor) branch of the ulnar nerve: A detailed examination of its course and the clinical significance of its damage. J Hand Surg Eur Vol 2009;34:47-57. [Google Scholar] |
| 12. | Midha R. Serrano-Almeida C. Mackay M. 69 harvesting techniques of cutaneous nerves for cable graft repair. In: Spine and Peripheral Nerves. 2nd ed. Stuttgart: Georg Thieme Verlag; 2007. Available from: http://www.thieme-connect.de/products/ebooks/lookinside/10.1055/b-0034-84038. [Last accessed on 2018 Dec 18]. [Google Scholar] |
| 13. | Colbert SH, Mackinnon SE. Nerve transfers for brachial plexus reconstruction. Hand Clin 2008;24:341-61, v. [Google Scholar] |
| 14. | Ray WZ, Yarbrough CK, Yee A, Mackinnon SE. Clinical outcomes following brachialis to anterior interosseous nerve transfers. J Neurosurg 2012;117:604-9. [Google Scholar] |
| 15. | Brown JM, Mackinnon SE. Nerve transfers in the forearm and hand. Hand Clin 2008;24:319-40, v. [Google Scholar] |
| 16. | Ray WZ, Chang J, Hawasli A, Wilson TJ, Yang L. Motor nerve transfers: A comprehensive review. Neurosurgery 2016;78:1-26. [Google Scholar] |
| 17. | Bertelli JA, Ghizoni MF. Results and current approach for brachial plexus reconstruction. J Brachial Plex Peripher Nerve Inj 2011;6:2. [Google Scholar] |
| 18. | Nunley JA, Ugino MR, Goldner RD, Regan N, Urbaniak JR. Use of the anterior branch of the medial antebrachial cutaneous nerve as a graft for the repair of defects of the digital nerve. J Bone Joint Surg Am 1989;71:563-7. [Google Scholar] |
| 19. | Mokhtee DB, Brown JM, Mackinnon SE, Tung TH. Reconstruction of posterior interosseous nerve injury following biceps tendon repair: Case report and cadaveric study. Hand (N Y) 2009;4:134-9. [Google Scholar] |
| 20. | Higgins JP, Fisher S, Serletti JM, Orlando GS. Assessment of nerve graft donor sites used for reconstruction of traumatic digital nerve defects. J Hand Surg Am 2002;27:286-92. [Google Scholar] |
| 21. | Lowe JB 3rd, Maggi SP, Mackinnon SE. The position of crossing branches of the medial antebrachial cutaneous nerve during cubital tunnel surgery in humans. Plast Reconstr Surg 2004;114:692-6. [Google Scholar] |
| 22. | Stang F, Stollwerck P, Prommersberger KJ, van Schoonhoven J. Posterior interosseus nerve vs. medial cutaneous nerve of the forearm: Differences in digital nerve reconstruction. Arch Orthop Trauma Surg 2013;133:875-80. [Google Scholar] |
| 23. | Ansselin AD, Davey DF. Axonal regeneration through peripheral nerve grafts: The effect of proximo-distal orientation. Microsurgery 1988;9:103-13. [Google Scholar] |
| 24. | Tarlov IM, Epstein JA. Nerve grafts: The importance of an adequate blood supply. J Neurosurg 1945;2:49-71. [Google Scholar] |
| 25. | Shibata M, Tsai TM, Firrell J, Breidenbach WC. Experimental comparison of vascularized and nonvascularized nerve grafting. J Hand Surg Am 1988;13:358-65. [Google Scholar] |
| 26. | Doi K, Kuwata N, Kawakami F, Tamaru K, Kawai S. The free vascularized sural nerve graft. Microsurgery 1984;5:175-84. [Google Scholar] |
| 27. | Rose EH, Kowalski TA, Norris MS. The reversed venous arterialized nerve graft in digital nerve reconstruction across scarred beds. Plast Reconstr Surg 1989;83:593-604. [Google Scholar] |
| 28. | Gu YD, Wu MM, Zheng YL, Li HR, Xu YN. Arterialized venous free sural nerve grafting. Ann Plast Surg 1985;15:332-9. [Google Scholar] |
| 29. | Bertelli JA, Ghizoni MF. Nerve transfers for elbow and finger extension reconstruction in midcervical spinal cord injuries. J Neurosurg 2015;122:121-7. [Google Scholar] |
| 30. | García-López A, Sebastian P, Martinez F, Perea D. Transfer of the nerve to the brachioradialis muscle to the anterior interosseous nerve for treatment for lower brachial plexus lesions: Case report. J Hand Surg Am 2011;36:394-7. [Google Scholar] |
Fulltext Views
2,693
PDF downloads
387




