Translate this page into:
Influence of time to surgery and pin fixation (lateral or crossed) on Flynn's criteria in Gartland type II and III supracondylar fracture: A retrospective study on 129 patients
Corresponding Author:
William Dias Belangero
800 Dr. Emilio Ribas Street, Apartment 01, Campinas, Sao Paulo, CEP 13025141
Brazil
belangerowd@gmail.com
| How to cite this article: Moratelli L, Santarosa HM, Katayama AY, Belangero WD. Influence of time to surgery and pin fixation (lateral or crossed) on Flynn's criteria in Gartland type II and III supracondylar fracture: A retrospective study on 129 patients. J Musculoskelet Surg Res 2019;3:342-345 |
Abstract
Objectives: There is a lack of consensus about the ideal pin configuration (lateral vs. crossed) and time to surgery regarding supracondylar fractures. We aim in this study to evaluate the influence of pin configuration and time to surgery on the outcome, using the Flynn criteria. Methods: Retrospective study of all children with supracondylar humerus fracture (SCF) Gartland types II and III treated in a single center from 2007 to 2017. Outcomes were classified as satisfactory or unsatisfactory according to Flynn's criteria at 6 weeks after surgery. Demographic, clinical, and surgical characteristics, as well as complications, were analyzed. Inferential analysis was performed by Pearson's correlation coefficient or Fisher's exact test for categorical variables when indicated. Results: One hundred and twenty-nine patients met the inclusion criteria. Mean patient age was 6.3 ± 2.5 years old, and 59.7% were males. Gartland type III fractures accounted for 57.4% of cases. Satisfactory outcomes occurred in 60.5% during this period. There was no difference in outcomes between the type of fixation and time to surgery. All cases of iatrogenic ulnar nerve injury occurred with crossed pin configuration. Conclusion: Lateral or cross fixation and time to surgery do not influence functional outcomes after surgical treatment of SCF in children, but lateral fixation decrease the risk of ulnar nerve injury.Introduction
Supracondylar humerus fracture (SCF) is the most common elbow fracture and the second most common pediatric fracture overall.[1] Extension type fracture represents up to 95% of cases, classified by Gartland as types I and III according to the severity of displacement.[2] Leitch et al. included type IV fracture, characterized as an unstable fracture in both flexion and extension due to an incompetent periosteal hinge circumferentially, which has an impact on treatment.[3],[4]
Closed reduction and percutaneous pinning is the treatment of choice for Gartland types II and III when surgery is indicated, but no consensus exists over the ideal pin configuration (lateral vs. crossed) and time to surgery.[5],[6] Brazilian orthopedic surgeons use cross-pin fixation in 70.7% of Gartland type II fractures and 74.8% of Gartland type III fractures, despite the risk of ulnar nerve injury.[7]
The aim of this study was to evaluate the influence of pin configuration and time to surgery on outcomes, measured by Flynn's criteria, 6 weeks after surgery for types II and III SCFs.
Subjects and Methods
All medical records of pediatric SCF classified by Gartland as type II and type III and surgically treated from 2007 to 2017 were enrolled following the STROBE reporting tool. Multiple fractures and patients with insufficient data were excluded from the study. Standard treatment for this type of fracture is followed by all staff surgeons in the department. Closed reduction and pin fixation (two lateral divergent or crossed) were carried out under general anesthesia, followed by plaster immobilization with the forearm in a neutral position. Patients were discharged within 24 h after surgery. Follow-up visits took place at 7 and 15 days, postoperatively, with clinical and radiological evaluation. After 4 weeks, wires were removed and the plaster cast was left for another 2 weeks. Following cast removal, the elbow range of motion and carrying angle was measured, and physiotherapy was recommended until the patient was able to perform normal daily living activities.
The following parameters were recorded: date and time of trauma, age (years and months), gender, side of fracture, Gartland classification, preoperative neural deficit, associated injuries, compartment syndrome, pin configuration (lateral or crossed), time to surgery, duration of surgery, surgical complication (iatrogenic nerve injury and return to operating room) pin site infection, and range of motion at 6 weeks after surgery. When the exact time of trauma could not be determined, emergency screening time was used.
The unsatisfactory outcome was defined by Flynn's criteria for the functional and cosmetic assessment of SCF treatment: loss of motion >15° or carrying-angle loss >15°. The overall rating was considered the lower of two ratings, and cubitus varus was automatically classified as unsatisfactory.[8] To avoid loss to follow-up and the impact of missing data – and ensure a comparison between patients at the same stage – range of motion was measured 6 weeks after surgery, when all devices (pin and splint) had been removed.
Complications were described from a surgical perspective and defined as iatrogenic nerve injury and need of reoperation (unsatisfactory reduction or loss of reduction). Time to surgery was classified as early (a period of 8 h after trauma) or late (more than 8 h).
Inferential analysis based on Flynn's criteria was performed by Pearson's correlation coefficient or Fisher's exact test for categorical variables when indicated. For numerical variables, Student's t-test or Mann–Whitney U-test were performed according to Shapiro–Wilk normality test result.
The analysis was performed using IBM® SPSS® Statistics version 24.0 for Windows software (Armonk, NY, USA), assuming a significance level of 5%.
Results
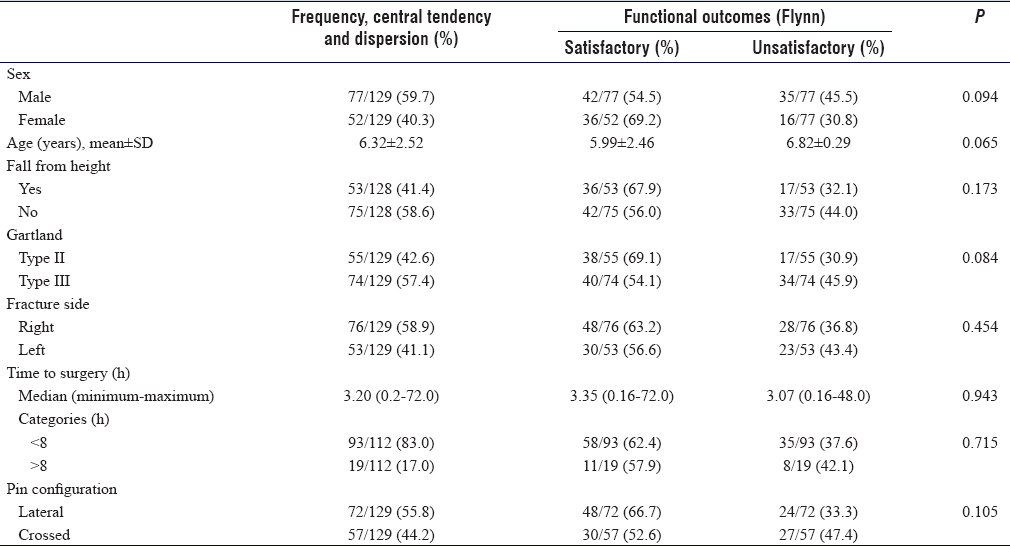
One hundred and twenty-nine patients met the inclusion criteria. Mean patient age was 6.3 ± 2.5 years old, and 59.7% of the patients were males. The main mechanism of trauma was a fall from height (58.6%), and the majority of patients underwent surgery within 8 h (83.0%) after the injury. There were no cases of flexion-type SCF. Gartland type III fractures accounted for 57.4% of cases. There was no difference between Gartland type II and III fractures in terms of age (P = 0.576), duration of surgery (P = 0.133), and pin configuration (P = 0.123).
Satisfactory outcomes occurred in 60.5% of cases. According to Flynn's criteria, there was no difference in outcome between Gartland classification, pin configuration, and time to surgery. There was also no difference between demographic, trauma, and surgical characteristics, as summarized in [Table - 1].
![[Table - 1]](#tbl_SaudiOrthopJ_2019_3_4_342_265827_t1.jpg){kind=link}
Seven patients had associated injuries. One with an absent radial pulse which returned after fracture reduction, four with radial nerve injuries, defined as neuropraxia which resolved spontaneously after a few weeks, and two patients had compartment syndrome caused by high-energy trauma requiring fasciotomy. All patients achieved complete clinical recovery. No case of anterior interosseous nerve (AIN) palsy was detected.
Eight patients (6.2%) had surgical complications, including 5 (3.9%) with loss of reduction and 3 (2.3%) with ulnar nerve palsy after cross-pin fixation. All cases underwent reoperation to improve reduction or change pin configuration from cross to lateral divergent pin configuration. There were no records of infection.
Discussion
Flynn criteria are a common outcome measure used to assess SCF in children. Excellent results have been described in 84.8% of cases of Gartland type II and III fractures within 8–30 weeks after injury.[9] In contrast to those authors, the current study used Flynn criteria 6 weeks after surgery in all children to ensure a uniform comparison of criteria and to avoid the impact of loss to follow-up, a frequent occurrence in our setting. As a consequence of the short follow-up period, we found a lower overall percentage of satisfactory results (60.5%) compared to the literature, which is expected since an improvement in range of motion is expected within a few weeks.
Clinical and biomechanical studies have shown that the cross-pin configuration did not improve stability compared to a lateral pin configuration, but the medial approach may increase the risk of ulnar nerve injury.[6],[10] Moreover, in children with peripheral nerve injury related to SCF, Kwok et al. showed that 10.8% were K-wire-related iatrogenic injuries (details of the damaged nerves were not given).[11] In the present study, the K-wire configuration did not influence outcomes either, and there were three cases of iatrogenic ulnar nerve injury. All cases were associated with the cross-pin configuration.
To increase safety in cross-pin configuration, the ulnar nerve can be further protected not only by nerve palpation during medial pin insertion but also by making a small incision under direct visualization of the medial epicondyle.[12],[13],[14] In addition, it has been reported that many other strategies may reduce the incidence of iatrogenic ulnar nerve injury, for example, less elbow flexion, ultrasound-guided intervention, and intraoperative nerve monitoring.[15],[16],[17]
Nevertheless, we believe that the exclusive lateral approach is the best way to avoid iatrogenic ulnar nerve injury during surgical treatment of SCF in children, and this approach should be preferred whenever possible. Furthermore, a recent meta-analysis reported that two cross-pin configurations have the highest risk of ulnar nerve injury, but questions whether the lateral pin configuration would be sufficient for adequate stability. Therefore, those authors recommend three lateral pin configuration instead of a crossed pin configuration.[18]
Time to surgery apparently did not influence functional outcomes, in agreement with other authors.[6],[19],[20],[21] The surgical procedure can be postponed to the next day in case of no pain after immobilization, intact soft tissues, and normal neurovascular status.[22] Therefore, it is recommended that these fractures are treated as the first case the next morning rather than late in the evening, when the staff may be more tired and prone to achieve less favorable results.[6],[23]
In a meta-analysis, Babal et al. reported AIN palsy and radial nerve palsy as the two most common peripheral nerve injuries in extension-type SCF at patient presentation.[24] However, our study did not identify any AIN lesion during the perioperative period, nor identified any motor deficit 6 weeks postoperatively. This may be explained by a lack of cutaneous sensory components in the AIN which makes identification of neural lesion more difficult at the time of patient arrival, and results in unnoticed cases of neuropraxia.[25]
One patient presented with an absent radial pulse which returned after fracture reduction. Chaturvedi et al. studied 21 consecutive closed pediatric SCF without any pulse, showing that peripheral pulse returned in 13 cases after reduction. Their study also demonstrated that capillary filling time and oxygen saturation are better prognostic markers than the peripheral pulse for pulseless limbs.[26]
This study has limitations. Its retrospective nature is the main limitation, with intrinsic susceptibility bias (selection bias). Finally, the follow-up period was relatively short. As a result, a lower percentage of satisfactory outcomes compared to the literature was found, especially since an improved range of motion is expected within a few more weeks.
Conclusion
A K-wire configuration and time to surgery do not influence functional outcomes after surgical treatment of SCF in children. Thus, a lateral fixation can be adopted to decrease the risk of iatrogenic ulnar nerve injury.
Ethical consideration
This study was approved by the local research ethics committee (Brazilian Certificate of Presentation for Ethical Appreciation N° 43707415.4.0000.5404).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
LM drafted the text, analyzed the data, and contributed to the conception and design of the article. HMS and AYK collected data, drafted the text, and contributed to the conception and design of the article. WDB conceived and designed the study and participated in drafting and revising the text. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
| 1. | Cheng JC, Ng BK, Ying SY, Lam PK. A 10-year study of the changes in the pattern and treatment of 6,493 fractures. J Pediatr Orthop 1999;19:344-50. [Google Scholar] |
| 2. | Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet 1959;109:145-54. [Google Scholar] |
| 3. | Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL, et al. Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am 2006;88:980-5. [Google Scholar] |
| 4. | Abzug JM, Herman MJ. Management of supracondylar humerus fractures in children: Current concepts. J Am Acad Orthop Surg 2012;20:69-77. [Google Scholar] |
| 5. | Alton TB, Werner SE, Gee AO. Classifications in brief: The Gartland classification of supracondylar humerus fractures. Clin Orthop Relat Res 2015;473:738-41. [Google Scholar] |
| 6. | Abbott MD, Buchler L, Loder RT, Caltoum CB. Gartland type III supracondylar humerus fractures: Outcome and complications as related to operative timing and pin configuration. J Child Orthop 2014;8:473-7. [Google Scholar] |
| 7. | Moreira RFG, Nishimi AY, Zanon EM, Rama TS, Ciofi RPL, Dobashi ET, et al. Cross-sectional study of Gartland II and III humerus supracondylar fracture treatment in childhood: Brazilian orthopedists' opinion. Rev Bras Ortop 2018;53:129-35. [Google Scholar] |
| 8. | Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years' experience with long-term follow-up. J Bone Joint Surg Am 1974;56:263-72. [Google Scholar] |
| 9. | Dekker AE, Krijnen P, Schipper IB. Results of crossed versus lateral entry K-wire fixation of displaced pediatric supracondylar humeral fractures: A systematic review and meta-analysis. Injury 2016;47:2391-8. [Google Scholar] |
| 10. | Larson L, Firoozbakhsh K, Passarelli R, Bosch P. Biomechanical analysis of pinning techniques for pediatric supracondylar humerus fractures. J Pediatr Orthop 2006;26:573-8. [Google Scholar] |
| 11. | Kwok IH, Silk ZM, Quick TJ, Sinisi M, MacQuillan A, Fox M, et al. Nerve injuries associated with supracondylar fractures of the humerus in children: Our experience in a specialist peripheral nerve injury unit. Bone Joint J 2016;98-B:851-6. [Google Scholar] |
| 12. | Abdel Karim M, Hosny A, Nasef Abdelatif NM, Hegazy MM, Awadallah WR, Khaled SA, et al. Crossed wires versus 2 lateral wires in management of supracondylar fracture of the humerus in children in the hands of junior trainees. J Orthop Trauma 2016;30:e123-8. [Google Scholar] |
| 13. | Kwak-Lee J, Kim R, Ebramzadeh E, Silva M. Is medial pin use safe for treating pediatric supracondylar humerus fractures? J Orthop Trauma 2014;28:216-21. [Google Scholar] |
| 14. | Maity A, Saha D, Roy DS. A prospective randomised, controlled clinical trial comparing medial and lateral entry pinning with lateral entry pinning for percutaneous fixation of displaced extension type supracondylar fractures of the humerus in children. J Orthop Surg Res 2012;7:6. [Google Scholar] |
| 15. | Woo CY, Ho HL, Ashik MBZ, Lim KB. Paediatric supracondylar humeral fractures: A technique for safe medial pin passage with zero incidence of iatrogenic ulnar nerve injury. Singapore Med J 2018;59:94-7. [Google Scholar] |
| 16. | Soldado F, Knorr J, Haddad S, Diaz-Gallardo P, Palau-Gonzalez J, Mascarenhas VV, et al. Ultrasound-guided percutaneous medial pinning of pediatric supracondylar humeral fractures to avoid ulnar nerve injury. Arch Bone Jt Surg 2015;3:169-72. [Google Scholar] |
| 17. | Shtarker H, Elboim-Gabyzon M, Bathish E, Laufer Y, Rahamimov N, Volpin G, et al. Ulnar nerve monitoring during percutaneous pinning of supracondylar fractures in children. J Pediatr Orthop 2014;34:161-5. [Google Scholar] |
| 18. | Na Y, Bai R, Zhao Z, Han C, Kong L, Ren Y, et al. Comparison of lateral entry with crossed entry pinning for pediatric supracondylar humeral fractures: A meta-analysis. J Orthop Surg Res 2018;13:68. [Google Scholar] |
| 19. | Kwiatkowska M, Dhinsa BS, Mahapatra AN. Does the surgery time affect the final outcome of type III supracondylar humeral fractures? J Clin Orthop Trauma 2018;9:S112-5. [Google Scholar] |
| 20. | Schmid T, Joeris A, Slongo T, Ahmad SS, Ziebarth K. Displaced supracondylar humeral fractures: Influence of delay of surgery on the incidence of open reduction, complications and outcome. Arch Orthop Trauma Surg 2015;135:963-9. [Google Scholar] |
| 21. | Han QL, Wang YH, Liu F. Comparison of complications and results of early versus delayed surgery for Gartland type III supracondylar humeral fractures in pediatric patients. Orthop Surg 2011;3:242-6. [Google Scholar] |
| 22. | Rupp M, Schäfer C, Heiss C, Alt V. Pinning of supracondylar fractures in children strategies to avoid complications. Injury 2019;50 Suppl 1:S2-9. [Google Scholar] |
| 23. | Murnaghan ML, Slobogean BL, Byrne A, Tredwell SJ, Mulpuri K. The effect of surgical timing on operative duration and quality of reduction in type III supracondylar humeral fractures in children. J Child Orthop 2010;4:153-8. [Google Scholar] |
| 24. | Babal JC, Mehlman CT, Klein G. Nerve injuries associated with pediatric supracondylar humeral fractures: A meta-analysis. J Pediatr Orthop 2010;30:253-63. [Google Scholar] |
| 25. | Cramer KE, Green NE, Devito DP. Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-5. [Google Scholar] |
| 26. | Chaturvedi H, Khanna V, Bhargava R, Vaishya R. Predictive factors determining outcomes in pulseless limb in paediatric supracondylar fractures of humerus. J Clin Orthop Trauma 2018;9:S92-6. [Google Scholar] |
Fulltext Views
1,609
PDF downloads
387




