Translate this page into:
Fractures caused by car accidents admitted to a tertiary care hospital: A cross-sectional study
Corresponding Author:
Abdulrahman S Alraddadi
Department of Basic Medical Sciences, College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, PO Box: 3660, Riyadh 11481
Saudi Arabia
raddadia@ksau-hs.edu.sa
| How to cite this article: Alraddadi AS, Al Muklass AM, Alhammad S, Alasmari A, Alhejji K, Alghathber N. Fractures caused by car accidents admitted to a tertiary care hospital: A cross-sectional study. J Musculoskelet Surg Res 2020;4:36-41 |
Abstract
Objectives: Car accidents (CAs) are considered as one of the leading causes of mortality worldwide. They cause various ramifications on individuals and society, with fractures being a major one. Because of poor local epidemiological data, economic burden, and the enormity of the outcomes of CA, the aim of this study was to provide vital statistics about the most frequent sites of fractures due to CA. Methods: This is a retrospective cross-sectional study conducted in King Abdulaziz Medical City, Riyadh, Saudi Arabia. It included individuals who were admitted to the hospital with fractures from CA. The study looked for bone fractures related to CA, the length of hospital stay, the age, and the gender of each individual. The data included all patients aged ≥15 years who were admitted to inpatient departments from January 2011 to December 2015. Results: A total of 1396 individuals were included, of which 86% were male. The median age of injured patients was 26 years. The median length of hospital stay was 10 days. The most common fracture found was in the acetabulum (10%). The most common region to be fractured was the skull (n = 376, 27%). Males were more predisposed to fractures in the acetabulum (11%) and the base of the skull (10%). Females were more prone to develop fractures in the pubis (10%) and the malar and maxillary bones (9%). Conclusions: The study showed that the young population has the highest number of fractures after CA, and these fractures are common in the acetabulum and skull.
Introduction
Car accidents (CAs) are considered as one of the leading causes of death worldwide.[1] The World Health Organization estimated that globally, 1.25 million deaths in 2013 were due to CAs, which means that every 25 s, a person dies from CAs.[1] CAs are not only a major cause of death worldwide but can also cause various ramifications on individuals, society, and economies. One example of those ramifications seen on a daily basis is injuries, including lacerations, fractures, and dislocations.[2] Fractures from CAs constitute up to a third of injuries with a high rate of morbidity.[2]
In Saudi Arabia, according to the statistics published by the Ministry of Interior-General Directorate of Traffic, 518,785 accidents occurred in 2015, an average of 1421 a day and 59 an hour.[3] The cost of these accidents reached more than 5 billion US dollars.[4] One of each five cases reported by the Saudi Red Crescent Authority is related to CAs.[4] For injuries, the average of the global percentage of injuries caused by CAs is estimated to be one injury from every eight cases, whereas locally, from every eight CAs, six resulted in injuries; that ratio is much higher than the global statistics.[4] In particular, Riyadh Province accounts for 28% of the total CAs in Saudi Arabia.[3] The proportion of the population in Riyadh accounts for 25% of the total population of Saudi Arabia.[3]
One of the chief causes of fractures is CAs. According to the American Academy of Orthopaedic Surgeons, CAs can cause different types of fractures ranging from minor to major.[5] However, international information about the predominant sites of fractures from CAs is not specific to either fractures alone or fractured bones. In 2002, a study conducted in China found the most common fracture arranged as follows: the lower limbs, the upper limbs, the skull, and the maxillofacial regions, and the least fractured area was the spine.[6] Another study conducted in Barcelona in 2000 found that neck sprains constituted the highest type of injuries among car occupants. On the other hand, bruises of the lower extremities were found most in motorcycle drivers and pedestrians, and upper extremities fractures were the most common with cyclists.[7]
Local research articles regarding CA injuries are few, lack specificity about the subject matter, or are not localized in Riyadh Province. An example of such articles is a research that was published in 2015, which discussed road safety and CAs in Almadinah Almunawwarah but did not specifically look for CA fractures and their patterns.[8] Another study published in 2013 from Riyadh and analyzed the patterns and etiology of maxilla fractures, but like many other research articles, it only concentrated on one specific region of the body.[9] Moreover, a study that looked at the epidemiology of fractures and dislocations among urban communities[10] showed that 41% of the injuries were due to road traffic and motorcycle accidents. This study, however, did not specify the type nor location of fracture among this 41%. There is a need for more research regarding the subject to be conducted in the capital of Saudi Arabia.[3]
Because of the poor local epidemiological data, the economic burden, the enormity of the outcome of CAs, and their effect on society, this study aimed to provide vital statistics about the most frequent sites of fractures in a tertiary hospital in Riyadh, Saudi Arabia. The significance of this research could help health-care providers to formulate which sites of the body are more commonly fractured and give a comparison between males and females, different age groups, and the length of stay (LOS). This study will hopefully aid many institutions, such as hospitals, the Riyadh Traffic Department, and car manufacturers, to improve their quality of safety measurements.
Subjects And Methods
The study was designed as a retrospective cross-sectional study and conducted at the King Abdulaziz Medical City in Riyadh, Saudi Arabia. The data included all patients who were admitted to the inpatient departments from January 2011 to December 2015 with fractures from CAs, and it was exclusive to individuals aged 15 years and above. After getting the institutional review board (IRB) approval, the investigators pulled out the patient data from the King Abdulaziz Medical City in Riyadh. The investigators looked for bone fractures related to CAs, the LOS in the hospital, the age, and the gender of each individual. The study relied on the coding system of the hospital, which uses the International Statistical Classification of Diseases and Related Health Problems 10 (ICD-10) for coding, for fractures and CAs. It gathered patients coded with both codes together in the duration of time determined and included them all in the study.
The data were analyzed using Microsoft Excel (2013) and IBM Statistical Package for Social Sciences version 25 (Armonk, NY, United States). Raw data were recoded into variables to answer the research questions, where the researchers assigned a separate variable for each fracture and body part. The analysis was done blindly, where codes were used for fractures and body parts, and then, these codes were transformed to their meanings in the final report.
The analysis report involved univariate and bivariate analyses. The univariate analysis included the frequencies and percentages of background characteristics of the study population (age distribution and gender composition) and fractures that the individuals had. The bivariate analysis included cross-analysis of the most common fractures by gender and age groups. For bivariate analysis, the appropriate statistical method was used to evaluate the statistical significance of the differences between variables groups (Chi-square test for categorical variables and analysis of variance for comparing means of multiple groups). The generated P values were evaluated for statistical significance, where values <0.05 were considered statistically significant.
Results
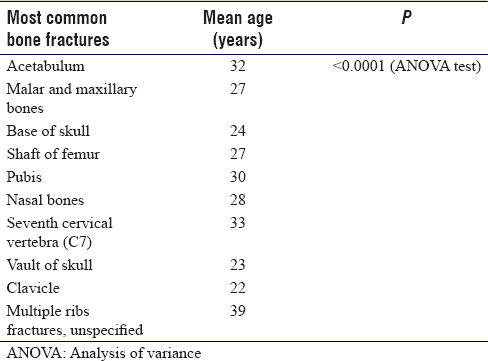
A total of 1396 individuals (86% were male) who had fractures due to CAs were included in this study, with a total number of 3202 fractures. The average number of fractures per person was 2.3. The median age of injured patients was 26 (20–37) years. The median length of hospital stay was 10 (5–23) days [Figure - 1]. The study found that the most common fractures resulting from CAs were fracture of the acetabulum (10%), malar and maxillary bones (9%), base of the skull (9%), shaft of femur (9%), and pubic bone (7%). Furthermore, the study found that there was a statistical difference in the mean age at which the patients get fractures depending on the bone, P < 0.0001 [Table - 1].
![[Figure - 1]](#fig_SaudiOrthopJ_2020_4_1_36_275174_f1.jpg){kind=link}
![[Table - 1]](#tbl_SaudiOrthopJ_2020_4_1_36_275174_t2.jpg){kind=link}
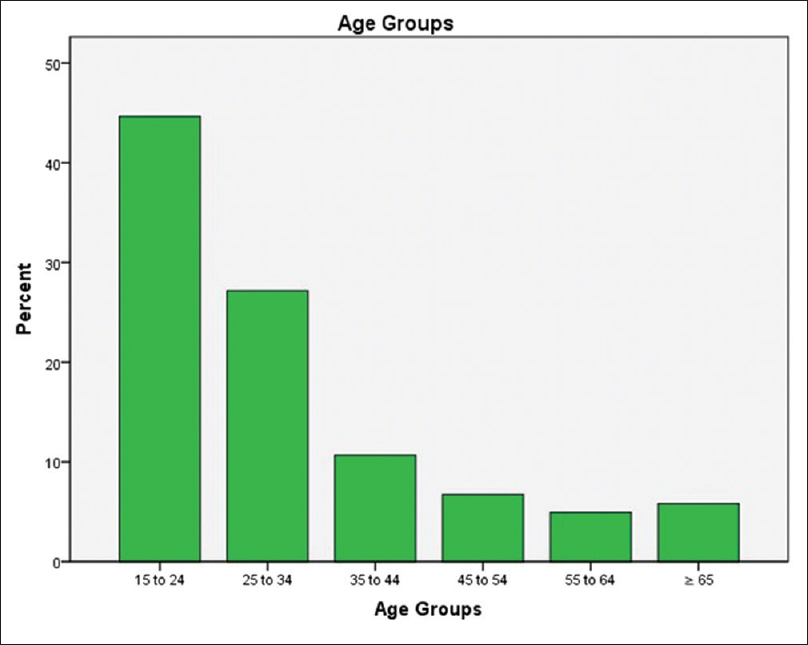 |
| Figure 1: The age group distribution of car accident patients included in the study |
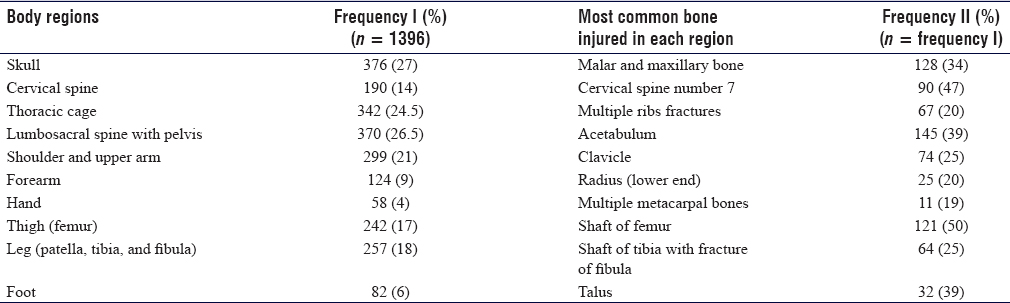
In addition, when the body was divided depending on ICD-10 general classification, the results showed that the body regions most commonly fractured were as follows: skull (27%), lumbar vertebra with pelvis (26.5%), thoracic cage (24.5%), and shoulder and arm (21%), followed by leg “patella, tibia, and fibula” (18%) [Table - 2].
![[Table - 2]](#tbl_SaudiOrthopJ_2020_4_1_36_275174_t3.jpg){kind=link}
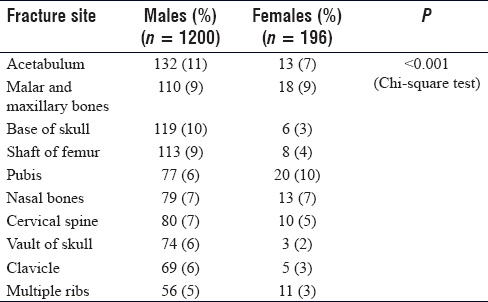
Concerning gender, males were more predisposed to be fractured in these parts: acetabulum (11%), followed by the base of skull fracture (10%), the shaft of femur (9%), malar and maxillary bones (9%), and cervical spine (C7; 7%). Females were more prone to develop fractures in the following bones: pubic bone (10%), malar and maxillary bones (9%), acetabulum (7%), and nasal bones (7%) and to develop multiple rib fractures (6%), P < 0.001 [Table - 3].
![[Table - 3]](#tbl_SaudiOrthopJ_2020_4_1_36_275174_t4.jpg){kind=link}
Discussion
This study found the most commonly fractured bones from CAs in patients who were admitted into the hospital and found differences between their baseline characteristics. The most important factor leading to these results is that admitted patients tend to sustain more severe fractures with other concomitant injuries; thus, they have a special pattern of fractures and have longer periods of stay in hospitals. Other factors that could contribute to the findings of this study are the mechanism of the accident, including the peculiar points in the car where the bones might reside, the speed at which the accident happened, the location of the injured patient (driver or passenger), and whether the seatbelt was fastened or not.[11],[12] In addition, the structure of the car is considered a major determinant of injuries because of the differences in the distribution and severity of injuries between various types of cars.[13]
To compare the pattern of fractures with an older study, an article published in 1990 looking for the pattern of accidental fractures and dislocations in Saudi Arabia found that the most common fractures were radius and ulna followed by fractures of the hand bones, foot bones, tibia and fibula, humerus, clavicle, femur, ankle, spine, and pelvis, which differs greatly from our results.[14] This study assumes that the difference in outcomes could be for several reasons. For instance, this article discusses the sites of fracture that are found in patients who are admitted in the hospital from CAs specifically, whereas the other study's inclusion criteria were of wider scope and included both patients initially treated at the emergency department and the admitted ones. It was also not specific to CAs but included bicycle, motorcycle, and pedestrian accidents as well. Furthermore, the cars that were used in 1986 and the cars that were used in the duration of the current study and their safety features are different, which could affect the outcome of fractured bones after a crash occurs.
In addition, a study of road traffic accidents (RTAs) and fractures in Nigeria found that the most commonly fractured bone is the femur, followed by the tibiofibula, humerus, tibia, and then clavicle.[15] Moreover, another study conducted in India about the patterns of fractures and dislocations from RTA concluded that the most common fracture is multiple fractures in which more than two sites are involved, followed by the tibiofibula, hand, radius and ulna, humerus, and then foot.[16] This variance could be attributed to the fact that the two countries, Nigeria and India, are heavily reliant on motorcycles and other two-wheeled vehicles as modes of transportation, which are not commonly used in Saudi Arabia.[15],[16],[17]
This study found that acetabular fractures are the most common type of fractures in admitted patients after CAs. This finding can be linked to the way that the accidents happened since this type of fracture is associated with high-energy collisions.[18] This could reflect the reckless behaviors of the drivers and violation of traffic laws including speed limits.[8] In addition, it affects the same population as in the other studies, which shows that acetabular fractures are higher among males, with a similar mean age found in the studies by Maia et al. and Kumar et al., 33 and 39 years, respectively.[19],[20] Furthermore, this kind of fracture is difficult to treat compared to other types (upper and lower limbs) because it is associated with a higher rate of complications and injuries to adjacent structures such as neurovascular bundles, bladder, ureter, and intestine.[21] Naturally, this can increase the LOS in the hospital if the injuries happen or increase the likelihood of admission to exclude those injuries, even if the problem is confined to the bone itself. In addition, acetabular fractures need to be observed in the hospital for a longer period of time, especially if they are accompanied by other nonacetabular fractures because of high morbidity and mortality rates and the need for postoperative care and rehabilitation.[22]
In the gender comparison of fractures from CAs, this study found that 86% of the fractured patients were male, whereas 14% were female. This is contributed to the fact that females were not allowed to drive in the duration of this study.[23] In the 1986 study mentioned earlier, the results showed that 80% of the fractured patients were male, whereas 20% were female, which resembles our study to some degree.[14] In addition, a study carried out in India, where men are the main laborer in the working community, showed that 80% of patients with fractures resulting from CAs were male compared to 20% were female.[16] Moreover, Nigeria's study results showed that males accounted for 57% and females 43%.[15] It is believed that the incidence of fractured female patients from CAs is going to increase in the future since females are now allowed to drive in Saudi Arabia.
In the comparison of ages, this study has found that the most common ages at which people are fractured are between 15 and 34 years, which accounts for 72% of the study participants. A study done in Saudi Arabia with RTA being the most common cause of injury concluded that the mean age of injured patients was 31 ± 14.4 years.[24] In addition, a study conducted in Qatar found that the majority (69%) were in the age range of 20–44 years.[25] In Nigeria, a study reported that the majority of injured people in RTA ranged from 30 to 40 years old, whereas in India, a study found that the age of fractured people in RTA ranged from 15 to 30 years.[15],[16] It is believed that the carelessness of youngsters and nonstrict local traffic laws that cannot deter the underage from driving are the reasons for this study's results regarding the younger ages.[8]
RTAs have great effects on multiple domains health-related, economic, and social, so methods of prevention have been and will be implemented through the years. Prevention could start from the beginning, in terms of car manufacturing and better safety systems. Raising awareness about the consequences of reckless driving and casualty, in general, is one important aspect to focus on. In Saudi Arabia, there has been a recent update on the penalty for breaking the law.[26],[27] One important implementation for road traffic safety in Saudi Arabia is speed radar.[24] Another recent safety measurement, implemented in 2016–2018, is the detection of unfastened seatbelts and mobile phone usage while driving by radar camera.[27] This measurement has led to a major improvement in seatbelt compliance from 34% to 76%, leading to fewer complications, such as fractures, after CAs.[26],[27] Not only has seatbelt compliance increased, but also the usage of mobile phones while driving, which is considered one of the causes of CAs, has decreased from 14% to 10%.[27],[28]
One limitation of the current study was a single-based center study investigating only those admitted patients with severe injuries. Other limitations include lack information regarding the mechanism of accidents, positions inside the vehicles, types of vehicles, and patients' conditions in general. The study also did not discuss the types of fractures and the side of the affected bones. However, the current study recommends conducting further studies to include more medical centers and investigating other contributors to car accidents. This includes road safety and environmental factors such as crowds, volunteer involvement, and the response of health-care providers to the incidence from the accident place to the wards. Other factors such as position in the car, seat belt use, and airbag injury should also be considered in future studies to measure the impact of these factors on the resulted fractures. Looking also for adherence to the current safety measurements, studying the car types and the mechanisms of accidents could identify the source of the problem and contribute to decreasing the incidence of the issue or at least decreasing the severity and complexity of the fractures. Studying the geometry of the acetabulum and the impact of collision (direction of the collision and the biomechanical features of the injuries) could help in identifying vulnerable groups and establishing new technologies (besides the current safety methods) to prevent such fractures.[29]
Conclusions
Fractures caused by CAs were considered a major problem that affects individuals, especially those of a young age group (15–34 years). Males showed a different pattern of fractures compared to females. In addition, pelvic and skull areas were the most commonly affected and, in turn, could lead to longer stays in the hospital, increasing the economic burden on the facility and the country and affecting the quality of life for those patients and their families.
Recommendation
Finally, the current study could help health-care providers to formulate which sites of the body are more commonly fractured and correlate that with patients' baseline characteristics. Implementing more strict laws in regard to obtain a driver's license, deterrent penalties for reckless drivers, and increasing society's awareness about CA complications could help to improve this issue. With the recent legalization of women driving in Saudi Arabia, a follow-up study is recommended for the period 2016–2020.
Ethical considerations
The current study was ethically approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center at King Abdulaziz Medical City, Riyadh, Saudi Arabia (ID Number: SP17/299/R).
Acknowledgement
The authors appreciate the work of medical record services in King Abdulaziz Medical City and thank them for their cooperation in collecting the data. Special thanks to Dr. Mohammad Salah for participating in analyzing the data.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Authors' contributions
AR and AM conceived and designed the study and supervised the study generally. SA, AA, KH, and NG collected and organized data. All authors contributed in interpreting the analyzed data. SA, AA, KH, and NG wrote the initial draft of this manuscript. All authors have critically reviewed and approved the final draft of the manuscript and are responsible for the content and similarity index of the current manuscript.
| 1. | World Health Organization. Road traffic injuries. World Health Organization; 2016. Available from: https://www.who.int/en/news-room/fact-sheets/detail/road-traffic-injuries. [last accessed on 2019 Nov 28]. [Google Scholar] |
| 2. | Alfalahi E, Assabri A, Khader Y. Pattern of road traffic injuries in Yemen: A hospital-based study. Pan Afr Med J 2018;29:145.9. [Google Scholar] |
| 3. | General Authority for Statistics. Traffic accidents site by Region. General Authority for Statistics; 2015. Available from: https://www.stats.gov.sa/en/3465. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 4. | Riyadh Traffic. Moi.gov.sa; 2015. Available from: http://bit.ly/2pnt8mz. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 5. | Orthoinfo.aaos.org. Fractures (Broken Bones)-OrthoInfo – AAOS; 2012. Available from: http://orthoinfo.aaos.org/topic.cfm?topic=a00139. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 6. | Hou S, Zhang Y, Wu W. Study on characteristics of fractures from road traffic accidents in 306 cases. Chin J Traumatol 2002;5:52-4. [Google Scholar] |
| 7. | Ferrando J, Plasència A, Ricart I, Canaleta X, Seguí-Gómez M. Motor-vehicle injury patterns in emergency-department patients in a south-European urban setting. Annu Proc Assoc Adv Automot Med 2000;44:445-58. [Google Scholar] |
| 8. | Mansuri FA, Al-Zalabani AH, Zalat MM, Qabshawi RI. Road safety and road traffic accidents in Saudi Arabia. A systematic review of existing evidence. Saudi Med J 2015;36:418-24. [Google Scholar] |
| 9. | Abdullah WA, Al-Mutairi K, Al-Ali Y, Al-Soghier A, Al-Shnwani A. Patterns and etiology of maxillofacial fractures in Riyadh City, Saudi Arabia. Saudi Dent J 2013;25:33-8. [Google Scholar] |
| 10. | Sadat-Ali M, Alomran AS, Azam Q, Al-Sayed HN, Al-Dhafer BA, Kubarra AF, et al. Epidemiology of fractures and dislocations among urban communities of Eastern Saudi Arabia. Saudi J Med Sci 2015;3:54-7. [Google Scholar] |
| 11. | Meral O, Aktaş EÖ, Ersel M. Examination of morbidity and mortality of cases according to intra-vehicle position and accident mechanism. Ulus Travma Acil Cerrahi Derg 2018;24:216-23. [Google Scholar] |
| 12. | Ogundele OJ, Ifesanya AO, Adeyanju SA, Ogunlade SO. The impact of seat-belts in limiting the severity of injuries in patients presenting to a university hospital in the developing world. Niger Med J 2013;54:17-21. [Google Scholar] |
| 13. | Inamasu J, Kujirai D, Izawa Y, Kase K, Shinozaki H. Difference in severity and distribution of bodily injuries following collision between drivers of K-cars and standard vehicles. Injury 2019;50:205-9. [Google Scholar] |
| 14. | Shaheen MA, Badr AA, al-Khudairy N, Khan FA, Mosalem A, Sabet N. Patterns of accidental fractures and dislocations in Saudi Arabia. Injury 1990;21:347-50. [Google Scholar] |
| 15. | Igho O, Isaac O, Eronimeh O. Road traffic accidents and bone fractures in Ughelli, Nigeria. IOSR-JDSM 2015;14:21-5. [Google Scholar] |
| 16. | Kumar N. Pattern of fractures and dislocations in road traffic accident victims in a tertiary care institute of central India. IJSS 2016;15:21-3. [Google Scholar] |
| 17. | General Authority for Statistics. Chapter 14,Transportation. General Authority for Statistics; 2017. Available from: https://www.stats.gov.sa/en/943. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 18. | Mohammed O, Idris S. Patterns of pelvic and acetabular injury among Sudanese patients. SJMS 2010;4:375-84. [Google Scholar] |
| 19. | Maia MS, Santos DC, de Queiroga DM, de Oliveira Castro C, Silva RM, Reis AC, et al. Epidemiological analysis on acetabular fractures. Rev Bras Ortop 2011;46:23-6. [Google Scholar] |
| 20. | Kumar A, Shah NA, Kershaw SA, Clayson AD. Operative management of acetabular fractures. A review of 73 fractures. Injury 2005;36:605-12. [Google Scholar] |
| 21. | Helfet D. Pelvic Fractures/Acetabular Fractures. Hospital for Special Surgery; 2009. Available from: https://www.hss.edu/conditions_pelvic-fractures-acetabular-fractures.asp. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 22. | Phruetthiphat OA, Willey M, Karam MD, Gao Y, Westerlind BO, Marsh JL. Comparison of outcomes and complications of isolated acetabular fractures and acetabular fractures With associated injuries. J Orthop Trauma 2017;31:31-6. [Google Scholar] |
| 23. | Saudi Driving School. Saudi Driving School – Princess Nourah Bint Abdulrahman University; 2018. Available from: https://sds.pnu.edu.sa/sites/SDS_En/Pages/SDSHomePage.aspx. [Last accessed on 2019 Nov 28]. [Google Scholar] |
| 24. | Haddad SH, Yousef ZM, Al-Azzam SS, AlDawood AS, Al-Zahrani AA, AlZamel HA, et al. Profile, outcome and predictors of mortality of abdomino-pelvic trauma patients in a tertiary intensive care unit in Saudi Arabia. Injury 2015;46:94-9. [Google Scholar] |
| 25. | Bener A, Rahman YS, Mitra B. Incidence and severity of head and neck injuries in victims of road traffic crashes: In an economically developed country. Int Emerg Nurs 2009;17:52-9. [Google Scholar] |
| 26. | Alghnam S, Alkelya M, Alfraidy M, Al-Bedah K, Albabtain IT, Alshenqeety O. Outcomes of road traffic injuries before and after the implementation of a camera ticketing system: A retrospective study from a large trauma center in Saudi Arabia. Ann Saudi Med 2017;37:1-9. [Google Scholar] |
| 27. | Alghnam S, Towhari J, Alkelya M, Binahmad A, Bell TM. The effectiveness of introducing detection cameras on compliance with mobile phone and seatbelt laws: A before-after study among drivers in Riyadh, Saudi Arabia. Inj Epidemiol 2018;5:31. [Google Scholar] |
| 28. | Darzi A, Gaweesh SM, Ahmed MM, Novak D. Identifying the causes of drivers' Hazardous States using driver characteristics, vehicle kinematics, and physiological measurements. Front Neurosci 2018;12:568. [Google Scholar] |
| 29. | Holcombe S, Kohoyda-Inglis C, Wang L, Goulet JA, Wang SC, Kent RW. Patterns of acetabular femoral head coverage. Stapp Car Crash J 2011;55:479-90. [Google Scholar] |
Fulltext Views
3,993
PDF downloads
932




