Translate this page into:
Variety of hand surgery cases during the COVID-19 pandemic: Experiences from seven countries
2 Institute of the Hand, Clinic Bizet, Paris, France
3 Department of Orthopaedics, Division of Hand Surgery, Hospital Nacional Guillermo Almenara Irigoyen, Lima, Peru
4 Department of Orthopaedics and Traumatology, Division of Hand Surgery, Bursa Uludag University, Faculty of Medicine, Bursa, Turkey
5 Department of Orthopaedics, Hand Surgery Unit, CHIREC Site Delta Hospital, Brussels, Belgium
6 Hand Surgery Unit, Unidad Ortopedica de Colombia, Bogota, Colombia
7 Department of Orthopaedics, Division of Hand Surgery, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Corresponding Author:
Margareta Arianni
Ramsay Premier Bintaro Hospital, Jalan MH Thamrin No. 1, Bintaro Jaya Sektor VII, Tangerang Selatan, Banten
Indonesia
margarethuang2357@gmail.com
| How to cite this article: Arianni M, Arnaout A, Castro-Obeso JR, Cavit A, Cilli V, Medina J, Okhovatpour MA, Yilmaz K. Variety of hand surgery cases during the COVID-19 pandemic: Experiences from seven countries. J Musculoskelet Surg Res 2021;5:15-23 |
Abstract
Objectives: The COVID-19 pandemic has affected the practice of hand surgery in the world. The aim of this study is to learn and describe the variety of operated hand surgery cases between countries during the pandemic. Methods: Eight authors from seven countries collected data of hand surgery patients that they operated on within a 1-month study period. Age, gender, diagnosis, procedure, mechanism of injury, object causing injury, place of injury occurrence, type of anesthesia, and COVID-19 screening were recorded for emergency patients. We also noted the reasons for elective surgeries during the pandemic. Results: A total of 124 operated emergency patients and 19 elective patients from all 8 hand surgeons in 7 countries were reported within the study period. Fractures were found in 33.1% of 124 emergency patients, soft-tissue injuries in 39.5% of patients, combined fracture and soft-tissue injuries in 25% of patients, and infection in 3 patients. The most frequent mechanism of injury was the blunt mechanism (49.2%). Home and workplace injuries were 44.4% and 30.6% of emergency cases, respectively. Turkey presented the highest number of emergency patients (71 patients). Most injuries occurred in workplaces (49.3%) and homes (42.3%), with the predominance of penetrating mechanism of injury (47.9%). Excluding Turkey the other six countries were grouped, home and road injuries were the highest (47.2% and 37.7%, respectively). Elective hand surgeries were performed in only four countries. Implant removal (seven patients) was the most frequently performed. No patient was diagnosed with COVID-19. Conclusions: Hand surgery cases during the pandemic differed between institutions represented in this study, due to differences in restriction policies, demographics, and types of hospital. The surgical resources for possible outbreaks in the future must be prepared accordingly.
Introduction
The COVID-19 pandemic has affected the practice of hand surgery across the globe.[1],[2] With people less inclined to go out as restrictions were imposed, we generally saw a reduction in the number of operated cases in the field of hand surgery.[2] As pandemic and subsequent lockdowns also changed the behaviors and habits of the society, patterns of hand injury could have changed as well. The purpose of our study is to learn and describe the variety and frequency of operated hand surgery cases during the COVID-19 pandemic and related restrictions, as reported by eight hand surgeons in seven different countries. Our study may also serve as a future reference for injury prevention.
Materials and Methods
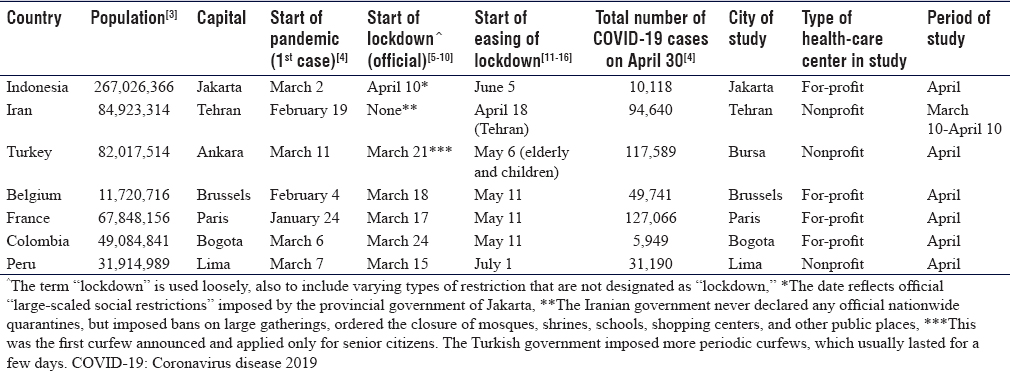
Eight hand surgeons in seven different countries (Indonesia, Iran, Turkey, Belgium, France, Colombia, and Peru) were offered and agreed to participate in this study. All participants retrospectively collected data of hand surgery patients that they had operated on during 1 month within the COVID-19 pandemic. Since the onset of COVID-19 outbreaks and implemented restrictions varied between countries, the beginning of the study time frame also differed between participants. Each participant determined their own study period. The study period must coincide with the strictest restrictions, or lowest mobility in the society, or peak of the pandemic, and must be before the alleviation of restrictions. Although the restrictions in many countries represented in this study may have lasted for more than 2 months, a 1-month study period was chosen for the sake of uniformity, and also because near the end of lockdown, people started to venture out and evade restrictions. The demographics and COVID-19 pandemic profiles of the seven countries[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16] are presented in [Table - 1]. Inclusion criteria included all cases operated by the eight participating hand surgeons during the determined study period. Exclusion criteria were as follows: (1) patients with procedures done outside the operating theater; (2) cases that were not within the field of hand and upper-limb surgery, despite being operated by hand surgeons (e.g., ankle fracture); and (3) patients whose affected or operated body regions were not stated in the diagnosis (e.g., osteomyelitis).
![[Table - 1]](#tbl_SaudiOrthopJ_2021_5_1_15_309927_t3.jpg){kind=link}
Operating theater data within the determined study period were retrospectively collected, and subcategorized into two categories: emergency and elective cases. Each participant should be involved in the surgery of the patients in the collected data. The patient's age, gender, diagnosis, treatment, COVID-19 screening status, and type of anesthesia used were recorded. Personal information was never obtained. For elective surgical cases, we noted the reason for surgery during the pandemic. For each emergency case, the following parameters were recorded: mechanism of injury, objects causing injury, place of occurrence, and background or etiology. Mechanism of injury, objects causing injury, and place of occurrence are, in fact, components or core modules of the International Classification of External Causes of Injury (ICECI). ICECI is a classification system that enables a systematic description of how injuries occur, which is designed specially to assist in injury prevention.[17] It has five core modules, namely intent (C1), mechanism of injury (C2), object/substance producing injury (C3), place of occurrence (C4), and activity when injured (C5). We realized that full, hierarchical, complete ICECI coding for our study's trauma cases would not be feasible. However, due to the fact that there are varying classifications for injury mechanism, we decided to adopt some aspects for the ICECI for uniformity and practicality. We used only up to two levels of the mechanism of injury module of the ICECI, but without numeric coding, as our aim was not to code the mechanism of injury. For example: “heavy stone falling onto the right hand” would be officially coded in ICECI as C2 1.2.3 (blunt force, contact with an object, and falling object, respectively), but in our study, we described it as “blunt (contact with an object),” simply to identify the mechanism of injury.
Analysis of emergency case data was presented in several schemes: (1) all seven countries combined, (2) six countries without Turkey, and (3) seven countries separately. We created scheme no. 2 because the high number of patients from Turkey's participants would serve as bias.
Results
Eight hand surgeons from seven countries had participated in this study. Four surgeons had practices in for-profit (private) health-care centers (Colombia, Belgium, France, and Indonesia), while the others had practices in nonprofit (academic) hospitals (Iran, Peru, and Turkey). Eight patients were excluded from this study because they had undergone procedures outside the operating theater. After this exclusion, all eight hand surgeons reported a total of 143 surgeries during the study period, 124 of which (86.7%) were emergency and 19 of which (14.8%) were elective. Screening protocols also varied between countries and health-care centers. Reverse-transcription polymerase chain reaction (RT-PCR) assays for SARS-CoV-2 were not ubiquitous in some countries in April 2020. Participant from Indonesia used routine chest computed tomography (CT) scans for all preoperative patients for detection of ground-glass opacities, which, if present, were then presumed as COVID-19. Participants from Belgium and Peru used RT-PCR assays for screening. Participants from Iran, France, Turkey, and Colombia relied only on clinical symptoms suspicious of COVID-19, which, if present, would then necessitate chest radiographs or chest CT scan. None of the patients recorded in this study was diagnosed with COVID-19.
Emergency surgery
A total of 124 emergency patients (40 females and 84 males) from all seven participating countries were reported. The mean age was 36.83 years (standard deviation = 18.65). Isolated fractures were found in 41 patients (33.1%), soft-tissue injuries in 49 patients (39.5%), and infection in 3 patients (2.4%). Twenty-five percent of emergency patients had combined fracture and soft-tissue injuries (e.g., digital amputation, tendon injury with metacarpal fracture, and fingertip injuries with distal phalanx fracture). Two patients of the isolated fracture group had injuries in at least two body regions: one case from Indonesia was a Galeazzi fracture with Le Fort III maxillary fracture, and one case from Iran was an elbow dislocation with distal radius fracture. Tendon injuries, either isolated or in conjunction with other injuries, were present in 40 patients (32.3%). Fourteen patients (11.3%) with nerve injuries and eight patients (6.5%) with arterial injuries requiring repair were recorded. Fingertip injuries were found in 26 patients (21%). The least common case reported was compartment syndrome (one patient). Two patients presented with postoperative wound infection and one patient presented with paronychia.
A variety of procedures performed are as follows. Open reduction and K-wire fixations were performed in 18 patients (14.5%), fixation with plate and screws in 25 patients (20.2%), external fixation in 1 case, and intramedullary nailing in 2 patients. Two fracture patients were treated with closed reduction and casts. There was only one arthroplasty performed in an emergency setting during the course of this study (comminuted radial head fracture from Belgium). Ten flaps (8.1%) were performed: four V-Y flaps, one crossed finger flap, two first dorsal metacarpal artery flaps, two innervated digital artery perforator flaps, and one homodigital island flap. Eleven cases of amputation (8.9%) were recorded – this consisted of six fingertip amputations not requiring replantation and five digital amputations requiring replantation (all of which were in Turkey). Ligament repair was reported in only one case (fourth CMC joint fracture-dislocation from Belgium), which was done in conjunction with internal fixation. There might have been other cases for which ligament repairs were performed as part of the main procedures, but not specifically reported, such as in replantation. One fasciotomy was performed for compartment syndrome. Debridement or drainage was performed in three patients.
A total of 61 patients (49.2%) with a blunt mechanism of injury were recorded [Figure - 1]. This included falls (25 patients), contact with an object (3 patients), contact with a person (1 patient), crush (18 patients), and transport injuries (12 patients). Injuries caused by machines, whether industrial or home machinery such as blender and washing machine, were classified separately as C2 3.2 (other mechanical force. contact with machinery) in ICECI. Therefore, we described this injury in this study as “other mechanical force (machinery),” which was the mechanism of injury in 12 cases (9.7%). Penetrating mechanism of injury (C2 2) was present in 48 cases (38.7%), which included one case of gunshot wound (C2 2.2.2). We did not subclassify penetrating injuries due to a lack of detailed description. As an example, “stabbed by a dagger” would be coded as C2 2.2.1 in ICECI (three levels), but in our study, it is simply described as “penetrating” (one level). We did not find mechanisms of injury other than the three mechanisms mentioned above. Five of the 13 transport injuries were found in Iran.
![[Figure - 1]](#fig_SaudiOrthopJ_2021_5_1_15_309927_f1.jpg){kind=link}
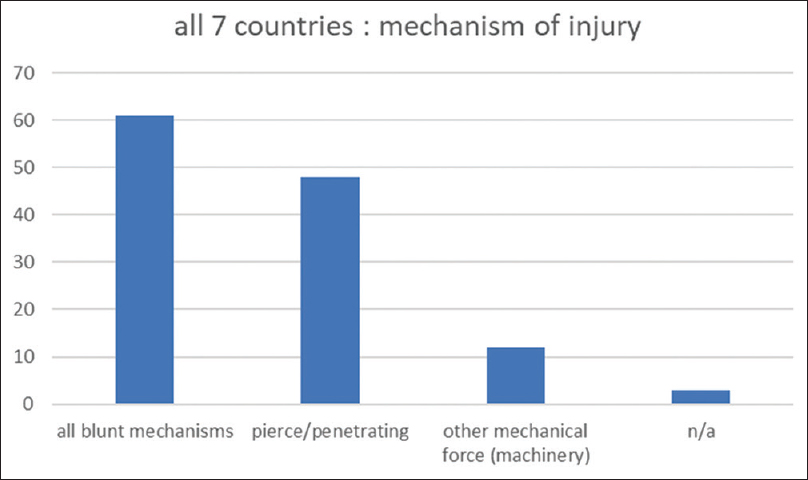 |
| Figure 1: Injury mechanism of emergency hand surgery patients from all authors in seven countries. Note: N/A: Not applicable – Patients for whom mechanism of injury was not applicable, e.g., infection |
The object causing injury, which is the third core module (C3) of ICECI, was mentioned whenever the object causing injuries, whether direct or indirect, was reported. We did not code the object causing injury but simply wrote down whatever was reported and whenever applicable. The knife was the object causing injuries in 14 cases. Other objects causing injury were as follows: saw (10 cases), axe (2 cases), glass – whether window or eating utensils (11 cases), and door (5 cases). Of the 12 injuries caused by machinery, electric polisher and cutting machine were identified as the objects causing injury in two patients. We did not specify the object causing injury in the 23 patients who had sustained injuries from falling, except for one patient whose fall was caused by an obvious reason (slippery bathroom floor). Fifty-five injuries (44.4%) took place in homes. Twenty-two injuries (17.7%) occurred on the roads, 38 (30.6%) in workplaces, and 6 (4.8%) in unspecified outdoor spaces [Figure - 2].
![[Figure - 2]](#fig_SaudiOrthopJ_2021_5_1_15_309927_f2.jpg){kind=link}
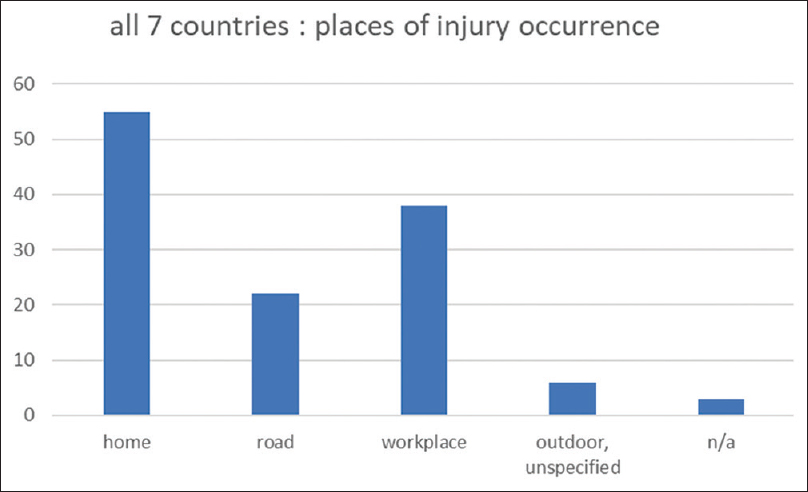 |
| Figure 2: Place of injury occurrence of emergency hand surgery patients from all authors in seven countries. Note: N/A: Not applicable – Patients for whom this category was not applicable, e.g., infection |
We identified seven self-inflicted injuries (5.6%), which consisted of one suicide attempt and six patients punching glasses in emotional states. One patient sustained an injury during an altercation. One patient from Peru sustained an injury from an accidental gunshot.
Regional anesthesia was the most frequently performed type of anesthesia in this study (63 surgeries, 50.8%). Local anesthesia was performed for 31 surgeries (25%) and wide-awake local anesthesia no-tourniquet (WALANT) for 4 surgeries. General anesthesia was performed in 25 surgeries (20.2%). Only one surgery was performed with intravenous sedation. Of all 25 patients who underwent general anesthesia, 13 patients were children (maximum age 14 years), 2 patients had multiple site involvement, and 3 patients had fractures of the shoulder girdle.
Six countries, excluding Turkey
When Turkey was excluded, and the other six countries were grouped together, we found that the most frequent mechanism of injury was the blunt mechanism (33 patients, 62.3%), in which fall was the most frequent mechanism within the blunt category (17 patients). Penetrating mechanisms accounted for injuries in 14 patients (26.4%). Injuries caused by machinery were documented in only three patients (5.6%). Fractures, whether isolated or in combination with other injuries, were present in 31 patients (58.5%). Tendon injuries and nerve injuries were reported in 8 (15.1%) and 6 (11.3%) patients, respectively. No arterial repair was reported. Most injuries in these six countries occurred in homes (25 patients, 47.2%) and on the roads (20 patients, 37.7%). Only three patients sustained injuries in workplaces, and two patients sustained injuries in outdoors.
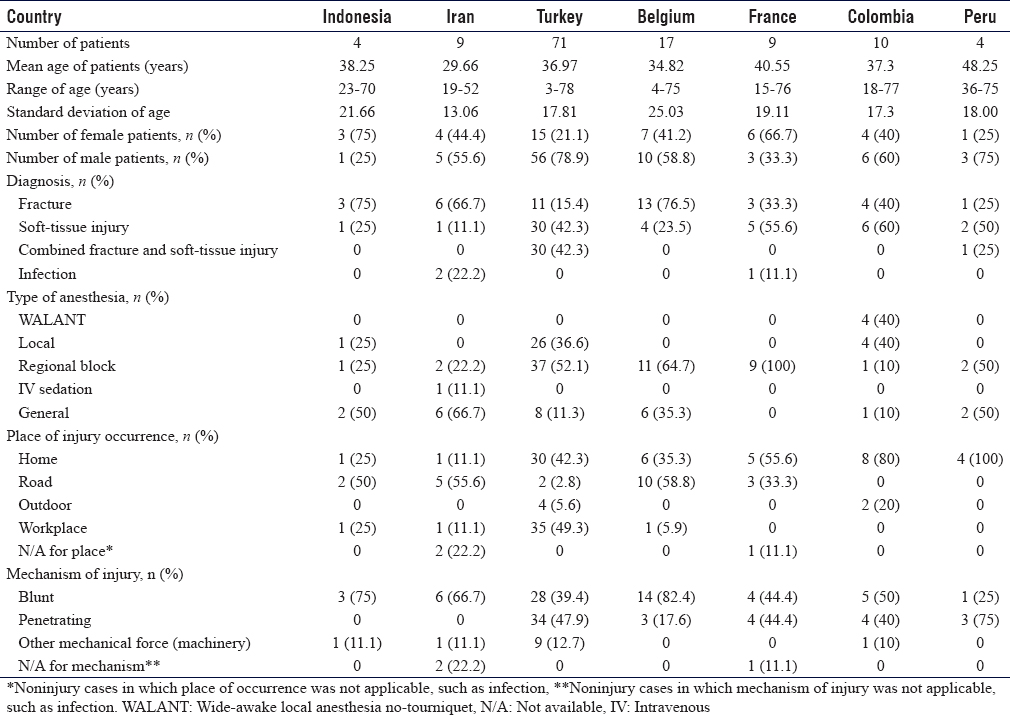
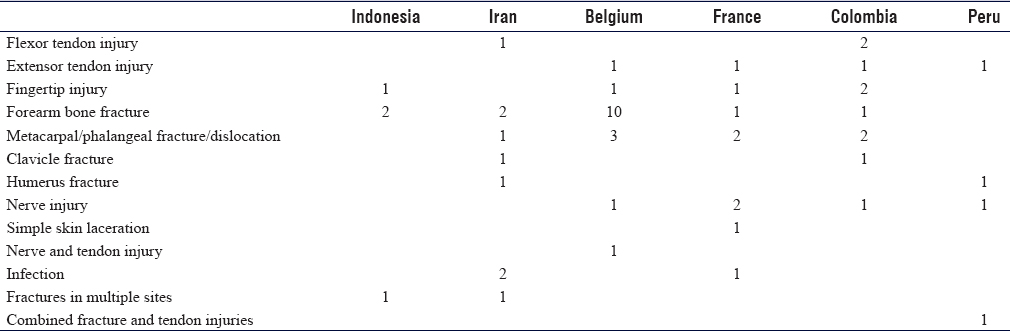
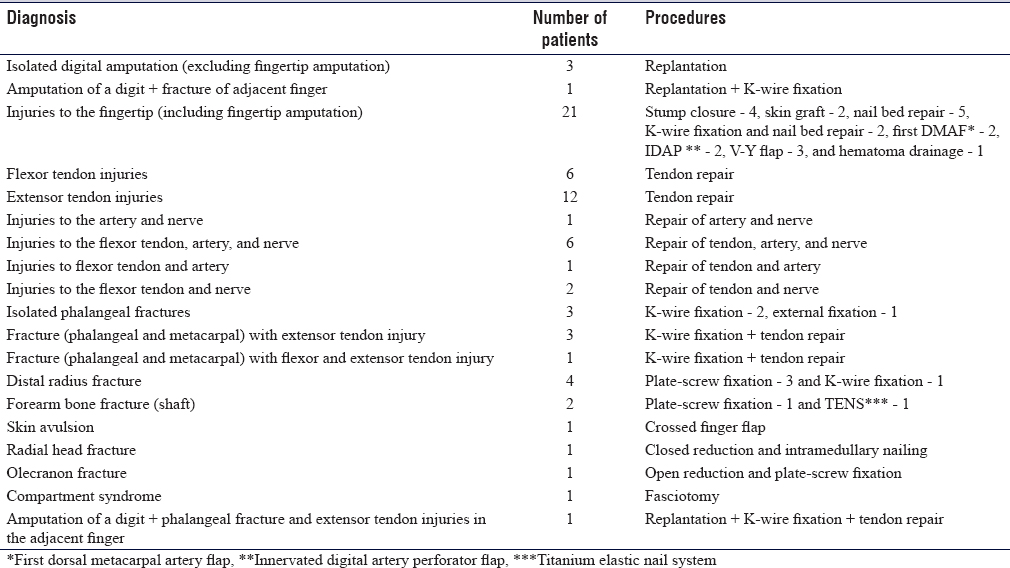
Our two participants from Turkey reported the highest number of emergency surgeries (a total of 71 surgeries). Participants from Indonesia and Peru reported the lowest number of emergency patients (four surgeries each). Participants from Iran, Belgium, France, and Colombia reported 9, 17, 9, and 10 emergency patients, respectively. The basic characteristics and varieties of emergency patients from each country are represented in [Table - 2] and [Table - 3], while the variety of emergency patients from Turkey is provided in [Table - 4].
![[Table - 2]](#tbl_SaudiOrthopJ_2021_5_1_15_309927_t4.jpg){kind=link}
![[Table - 3]](#tbl_SaudiOrthopJ_2021_5_1_15_309927_t5.jpg){kind=link}
![[Table - 4]](#tbl_SaudiOrthopJ_2021_5_1_15_309927_t6.jpg){kind=link}
Elective surgery
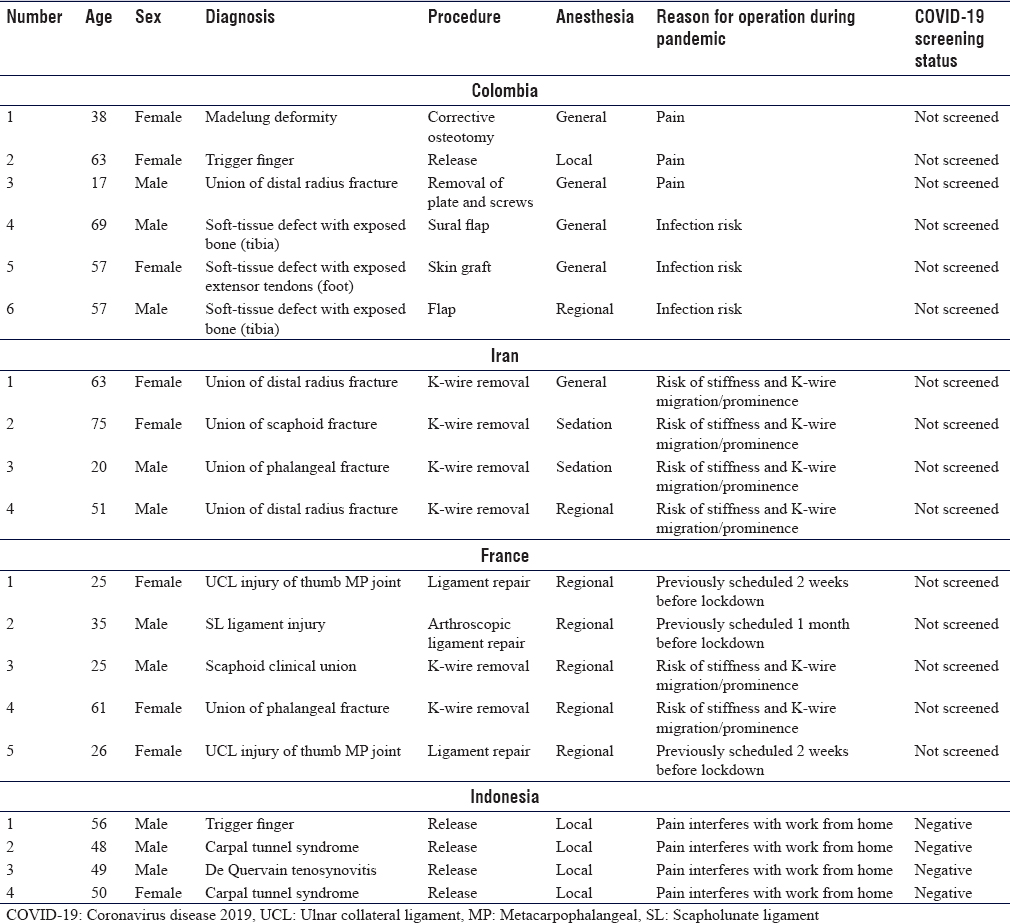
A total of 19 elective surgeries were performed by only 4 participants (Colombia – 6 surgeries, Indonesia – 4 surgeries, Iran – 4 surgeries, and France – 5 surgeries) during the course of study. There were 9 female patients and 10 male patients. There were a total of 7 implant removals (36.84%), 6 of which were removal of K-wires. Removal of plate and screws was performed in one patient (from Colombia), the reason of which being pain. Soft-tissue defect closures (flaps and skin grafts) were performed in three patients in Colombia. There were three cases of ligament injury from France for which repairs were performed (including one arthroscopic repair). These elective cases had been scheduled weeks before lockdown and were thus operated within the study period. Five patients with repetitive strain disorder were reported (two trigger fingers, one de Quervain tenosynovitis, and two carpal tunnel syndromes), all of which underwent release procedures. All four elective surgeries reported by the participant from Indonesia were release procedures for trigger finger, carpal tunnel syndrome, and de Quervain tenosynovitis. These patients demanded surgery due to pain that had interfered with their from-home works. One case of Madelung deformity was also operated on due to interfering pain. Overall, the main reason for elective surgery during the study period was pain (seven patients, 36.8%). Other reasons were K-wire-related problems (six patients, 31.6%) and infection risks (three patients, 15.8%).
Regarding anesthesia, regional anesthesia was the most frequently performed anesthesia (seven surgeries), followed by general anesthesia (five surgeries), local anesthesia (five surgeries), and intravenous sedation (two surgeries). Three of four participants doing elective surgeries during the study period had private practices. Participants from Peru, Turkey, and Belgium reported that elective surgeries were all postponed in their hospitals during the study period. [Table - 5] shows a more detailed presentation of elective surgical cases from the aforementioned four countries.
![[Table - 5]](#tbl_SaudiOrthopJ_2021_5_1_15_309927_t7.jpg){kind=link}
Discussions
Several studies conducted during the first few months of the pandemic showed the predominance of the number of home-related hand injuries. In a study by Régas et al.[18] in Nantes, France, domestic injuries accounted for 88.5% of all emergency hand injuries during the lockdown, while work injuries were only 10%. Pichard et al.[19] from Paris also reported a predominance of domestic hand injuries (66.5%) during the lockdown period; work-related injuries and road accidents were only 10% each. In our study, although home-related hand injuries apparently ranked first in percentage, they did not exceed 50%. Indeed, the variety of hand injuries varied between regions and populations. However, as our study made no direct comparison with prepandemic data, we could not conclude whether there were changes in the percentage of home-related hand injuries. Facchin et al.[20] from Northern Italy showed that the number of hand injuries was similar over a period of 3 years. They claimed to have witnessed only a slight relative increase in home-related injuries in 2020. Garude et al.[21] from Leeds compared cases of hand injuries during the early lockdown in March to April to those during the same months in the previous year. They found that there was no difference in the percentage of hand injury etiologies between 2019 and 2020, except for “injuries caused by tools at home,” which showed an increase in 2020. The more general term “domestic hand injuries,” workplace hand injuries, falls, and road traffic accidents did not show any difference between 2019 and 2020 (26% vs. 26%).[21] We speculate that the number of work-related hand injuries may have remained the same as before the pandemic in industrial towns or countries with less severe lockdown policy, and that in residential areas, the number of home-related hand injuries before and during the pandemic may not have differed.
Among the seven countries in this study, France was the first country to report its first COVID-19 case. However, Iran was the first country to have an outbreak that was followed by rapid local transmission, earlier than France.[4],[6] Therefore, participants from Iran defined the study period from March 10 to April 10 because businesses then started to reopen in mid-April 2020. The low number of patients reported by participants from Peru and Indonesia was due to the fact that the Almenara Hospital in Lima was “converted” into a specialized COVID-19 hospital, and that several health-care workers in Premier Bintaro Hospital passed away due to COVID-19, inciting fear from neighboring communities. The mobility of citizens in the greater Jakarta area was lowest in April 2020, particularly at the beginning of the fasting month of Ramadhan at the end of the month.[22] As we noted in [Table - 1], the official restrictions in Indonesia commenced later than the beginning of the study period. This is because there had been up to a 54% reduction in community mobility in Indonesia in late March.[23] Therefore, selecting April as the study period was deemed suitable. We admit that the numbers from Indonesian and Peruvian participants were too small to make any conclusions. Indeed, the unique situations affecting the aforementioned centers rendered them unsuitable to represent the region or nation. However, the small numbers reported reflected the real situation in the communities or districts served by both centers.
Our two participants from Turkey reported the highest number of emergency surgeries, as well as percentages of injury groups that were different from the other six countries. Indeed, when Turkey was excluded, there was a change in the percentage of injury groups. The uniqueness of cases from Turkey was accounted for by several factors: (1) the numbers came from the practice of two participants who work closely in a cohesive team; (2) during the pandemic, the curfew in Turkey did not follow the pattern adopted by most countries (the Turkish government adopted periodic curfews, which lasted for several days); (3) the city of Bursa is an industrial city; (4) and Uludag Hospital is the only hospital with hand surgery service in the area. In contrast to other participants in this study, participants from Turkey reported that in their practice, work-related hand injuries were predominant during the study period. Both participants made an anecdotal observation that the number of workplace injuries and hand emergency cases in their institution was similar to those before the pandemic. This notion is supported by several studies from Turkey before the pandemic. Kaya Bicer et al.[24] found that among all cases of emergency hand injuries in their series, 35% were occupational injuries. Davas Aksan et al.[25] reported that 76% of all hand injuries in their study were work related. The percentage of workplace hand injuries reported by our Turkish participants was somewhere between the two percentages provided by the two aforementioned studies.
The high percentage of workplace injuries reported by participants from Turkey may imply that in the event of future outbreaks and restrictions, the industrial sectors in industrial cities may continue to operate, particularly in regions or countries where restrictions are less tight. Therefore, resources for hand and microsurgery service (e.g., workforce, tools, and facilities) must be prepared accordingly as before the pandemic, as well as effective screening protocol for the high volume of patients and adequate personal protective equipment.
In Iran, restrictions in public transportation, the Nowruz (Persian New Year) holiday, and the fear of contracting COVID-19 in public transportation had encouraged people to use their own private vehicles.[26] This could have accounted for the fact that transport injury was predominant in our Iranian participant's practice.
Injuries sustained on the roads were the most prevalent cases reported by participants from Belgium; this fact implied that a part of the society in Brussels was still engaged in outdoor activities during the lockdown period. Participants from Belgium also reported that injuries sustained in workplaces were low in number. We could not conclude that this was accounted for by the lockdown itself as we did not compare the incidence of workplace injuries before and during the lockdown in the very same hospital.
Participant from France reported that penetrating home injuries were the most prevalent cases in her series during the study period. This finding seemed similar to those reported by Régas et al.,[18] Pichard et al.,[19] and Andrea et al.[27] – all of whom had reported a high percentage of domestic hand injuries during the pandemic-related restrictions. Still, we could not conclude that this was caused by the lockdown itself because several epidemiological studies before the pandemic had reported that home hand injuries were also predominant. For example, Nieminen et al.[28] reported that 70% of hand injuries had occurred at home. Trybus and Guzik[29] reported that 45% of hand injuries in their study had occurred at home. Ribak et al.[30] from Brazil also reported a high percentage of domestic upper-limb injuries (66%).
Our study has a certain degree of biases due to differences in the following aspects: (1) the onset of pandemic and restrictions, (2) the severity of the pandemic, (3) types and strictness of restrictions, (4) nationwide health-care policy, (5) hospital policy and hospital types, (6) duration of restriction, (7) easing of restriction, (8) study period between participants, (9) social behaviors in each country, (10) hand surgeons' experience and practice habits, and (11) the dynamic and ongoing nature of the pandemic. Other limitations in our study are that our study did not make comparisons between the incidence of hand surgery cases before and during the lockdown, and the lack of uniformity in reporting diagnosis and treatment. Some participants used the term “tendon transection,” while some others used the term “tendon injury.” Some details were also lacking, such as tendon injury zones and injured side (left or right), and not all institutions adopted ICD-10 coding. In addition, our application of the ICECI classification is far from perfect.
Despite the general expectations and one report stating that the WALANT technique was being employed more often since the beginning of the pandemic,[31] we did not find WALANT to be the predominant method of anesthesia. WALANT was performed only by the participant from Colombia. Different styles, habits, techniques, and policies between participants and their centers accounted for this finding.
Four participants in this study performed elective surgeries during the study period. We did not obtain information on the number of canceled elective surgeries during the study period that had been scheduled before restrictions. In this study, most elective surgery cases appeared to have time-sensitive issues or pain issues, which justified elective procedures despite the pandemic. It was also possible that private (for-profit) hospital policies played some roles, as three out of four hospitals facilitating elective surgeries in this study were private (for-profit).
Conclusion
This study is a snapshot of hand surgery practice in seven institutions in seven different countries during the early days of the COVID-19 pandemic. The large variations encountered in this study implied that the COVID-19 pandemic did not exert the same effect on hand surgery cases in all countries or institutions. Many factors that came into play, such as government policy, type of hospital, demographics in a particular district, and others, were reflected in this study's results. As the article is written, the pandemic is ongoing. Our study could contribute as a future reference in the preparation of resources needed during pandemic or lockdowns and in preventing hand injuries.
Ethical approval
This study was approved by the Ethical Committee of the Ramsay Premier Bintaro Hospital (001/KE/RSPB/XI/2020, November 1, 2020) and in accordance with the Declaration of Helsinki.
Financial support and sponsorship
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
There are no conflicts of interest.
Authors contribution
MA conceived and designed the study, acquired and organized data, and wrote the initial and final drafts of the study. AA, AC, and MAO designed the study, acquired and organized data, wrote parts of the draft, and approved the final draft of the study. JM, KY, VC and JRCO acquired and organized data, revised and approved the final draft of the study. All authors also critically reviewed and approved the final draft and are responsible for the manuscript's content and similarity index.
| 1. | Ducournau F, Arianni M, Awwad S, Baur EM, Beaulieu JY, Bouloudhnine M, et al. COVID-19: Initial experience of an international group of hand surgeons. Hand Surg Rehabil 2020;39:159-66. [Google Scholar] |
| 2. | Martin-Playa P, Calzacorta-Muñoz P, Aparicio Elizalde L, Carrera-Casal O, García Gutiérrez JJ. An overview of the situation of hand surgery in Spain during the peak of COVID-19 pandemic. Hand Surg Rehabil 2020;39:454-8. [Google Scholar] |
| 3. | The World Factbook 2020. Washington, DC: Central Intelligence Agency; 2020. Available from: https://www.cia.gov/library/publications/resources/the-world-factbook/index.html. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 4. | WHO Coronavirus Disease (COVID-19) Dashboard. Geneva: World Health Organization; 2020. Available from: https://covid19.who.int/. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 5. | Mashabi S. Daftar 18 Daerah Yang Terapkan PSBB, Dari Jakarta Hingga Makassar; April 20, 2020. Available from: https://nasional.kompas.com/read/2020/04/20/05534481/daftar-18-daerah-yang-terapkan-psbb-dari-jakarta-hingga-makassar?page=all. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 6. | Raoofi A, Takian A, Akbari Sari A, Olyaeemanesh A, Haghighi H, Aarabi M. COVID-19 pandemic and comparative health policy learning in Iran. Arch Iran Med 2020;23:220-34. [Google Scholar] |
| 7. | Kandemir A. Turkey Imposing Curfew for People Over Age 65. Bloomberg; March 22, 2020. Available from: https://www.bloomberg.com/news/articles/2020-03-21/turkey-imposing-curfew-for-people-over-age-65-at-midnight. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 8. | Coronavirus: What Are the Lockdown Measures Across Europe? April 14, 2020. Available from: https://www.dw.com/en/coronavirus-what-are-the-lockdown-measures-across-europe/a-52905137. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 9. | Gamba L. Colombia Announces Lockdown as Coronavirus Cases Surge. Anadolu Agency; March 23, 2020. Available from: https://www.aa.com.tr/en/americas/colombia-announces-lockdown-as-coronavirus-cases-surge/1773775. [Last accessed on 2020 Aug 03]. [Google Scholar] |
| 10. | Pemerintah Peru Lakukan Lockdown Dalam Menghadapi COVID-19; March 03, 2020. Available from: https://kemlu.go.id/lima/id/news/5606/pemerintah-peru-lakukan-lockdown-dalam-menghadapi-covid-19. [Last accessed on 2020 Aug 04]. [Google Scholar] |
| 11. | Detikcom T. Anies Perpanjang PSBB DKI Jakarta, Bulan Juni Jadi Masa Transisi. DetikNews; June 04, 2020. Available from: https://news.detik.com/berita/d-5040091/anies-perpanjang-psbb-dki-jakarta-bulan-juni-jadi-masa-transisi. [Last accessed on 2020 Aug 04]. [Google Scholar] |
| 12. | Basravi Z. Iran to Reopen Businesses as COVID-19 Lockdown Eased. Aljazeera; April 17, 2020. Available from: https://www.aljazeera.com/news/2020/04/iran-reopen-businesses-covid-19-lockdown-eased-200417132846820.html. [Last accessed on 2020 Aug 04]. [Google Scholar] |
| 13. | Kozok F. Turkey Eases Virus Measures after Declaring #missionaccomplished#. Bloomberg; May 28, 2020. Available from: https://www.bloomberg.com/news/articles/2020-05-28/after-declaring-missionaccomplished-turkey-eyes-end-to-curfews. [Last accessed on 2020 Aug 04]. [Google Scholar] |
| 14. | Coronavirus: How Lockdown is Being Lifted Across Europe; July 02, 2020. Available from: https://www.bbc.com/news/explainers-52575313. [Last accessed on 2020 Aug 11]. [Google Scholar] |
| 15. | Newbery E. Colombia Extends Quarantine Until May 25, But Relaxes Rules. The Bogota Post; May 05, 2020. Available from: https://thebogotapost.com/colombia-extends-quarantine-until-may-25-but-relaxes-rules/46398/. [Last accessed on 2020 Aug 11]. [Google Scholar] |
| 16. | Briceno F. Peruvians Fill the Streets as Lockdown Ends Despite New Infections.' TIME; July 02, 2020. Available from: https://time.com/5862495/peru-lockdown-ends/. [Last accessed on 2020 Aug 11]. [Google Scholar] |
| 17. | ICECI Coordination and Maintenance Group. International Classification of External Causes of Injuries (ICECI) Version 1.2. Adelaide: Consumer Safety Institute, Amsterdam and AIHW National Injury Surveillance Unit; 2004. Available from: . [Last accessed on 2020 Jun 04]. [Google Scholar] |
| 18. | Régas I, Bellemère P, Lamon B, Bouju Y, Lecoq FA, Chaves C. Hand injuries treated at a hand emergency center during the COVID-19 lockdown. Hand Surg Rehabil 2020;39:459-61. [Google Scholar] |
| 19. | Pichard R, Kopel L, Lejeune Q, Masmoudi R, Masmejean EH. Impact of the COronaVIrus Disease 2019 lockdown on hand and upper limb emergencies: experience of a referred university trauma hand centre in Paris, France. Int Orthop 2020;44:1497-501. [Google Scholar] |
| 20. | Facchin F, Messana F, Sonda R, Faccio D, Tiengo C, Bassetto F. COVID-19: Initial experience of hand surgeons in Northern Italy. Hand Surg Rehabil 2020;39:332-3. [Google Scholar] |
| 21. | Garude K, Natalwala I, Hughes B, West C, Bhat W. Patterns of adult and paediatric hand trauma during the COVID-19 lockdown. J Plast Reconstr Aesthet Surg 2020;73:1575-92. [Google Scholar] |
| 22. | Dewi NS. Kurva Mobilitas Penduduk VS Kurva COVID-19. Digination; July 12, 2020. Available from: http://www.digination.id/read/016446/kurva-mobilitas-penduduk-vs-kurva-covid-19. [Last accessed on 2020 Aug 04]. [Google Scholar] |
| 23. | Google LLC “Google COVID-19 Community Mobility Reports”. Available from: http://www.google.com/covid19/mobility/. [Last accessed on 2020 Apr 07]. [Google Scholar] |
| 24. | Kaya Bicer E, Kucuk L, Kececi B, Murat Ozturk A, Cetinkaya S, Ozdemir O, et al. Evaluation of the risk factors for acute occupational hand injuries. Chir Main 2011;30:340-4. [Google Scholar] |
| 25. | Davas Aksan A, Durusoy R, Ada S, Kayalar M, Aksu F, Bal E. Epidemiology of injuries treated at a hand and microsurgery hospital. Acta Orthop Traumatol Turc 2010;44:352-60. [Google Scholar] |
| 26. | Faridi S, Yousefian F, Niazi S, Ghalhari MR, Hassanvand MS, Naddafi K. Impact of SARS-CoV-2 on ambient air particulate matter in Tehran. Aerosol Air Qual Res 2020;20:1805-11. [Google Scholar] |
| 27. | Poggetti A, Del Chiaro A, Nucci AM, Suardi C, Pfanner S. How hand and wrist trauma has changed during covid-19 emergency in Italy: Incidence and distribution of acute injuries. What to learn? J Clin Orthop Trauma 2021;12:22-26. [Google Scholar] |
| 28. | Nieminen S, Nurmi M, Isberg U. Hand injuries in Finland. Scand J Plast Reconstr Surg 1981;15:57-60. [Google Scholar] |
| 29. | Trybus M, Guzik P. Obrazenia rak w regionie krakowskim [Hand injuries in the Krakow Region]. Chir Narzadow Ruchu Ortop Pol 2004;69:201-6. [Polish]. [Google Scholar] |
| 30. | Ribak S, de Oliveira EJ, Rosolino GP, Orru P, Tietzmann A. Epidemiology of traumatic injuries of the upper limbs in a university hospital. Acta Ortop Bras 2018;26:370-3. [Google Scholar] |
| 31. | Hwee J, Chiew J, Sechachalam S. The impact of coronavirus disease 2019 (COVID-19) on the practice of hand surgery in Singapore. J Hand Surg Am 2020;45:536-41. [Google Scholar] |
Fulltext Views
1,641
PDF downloads
582




